
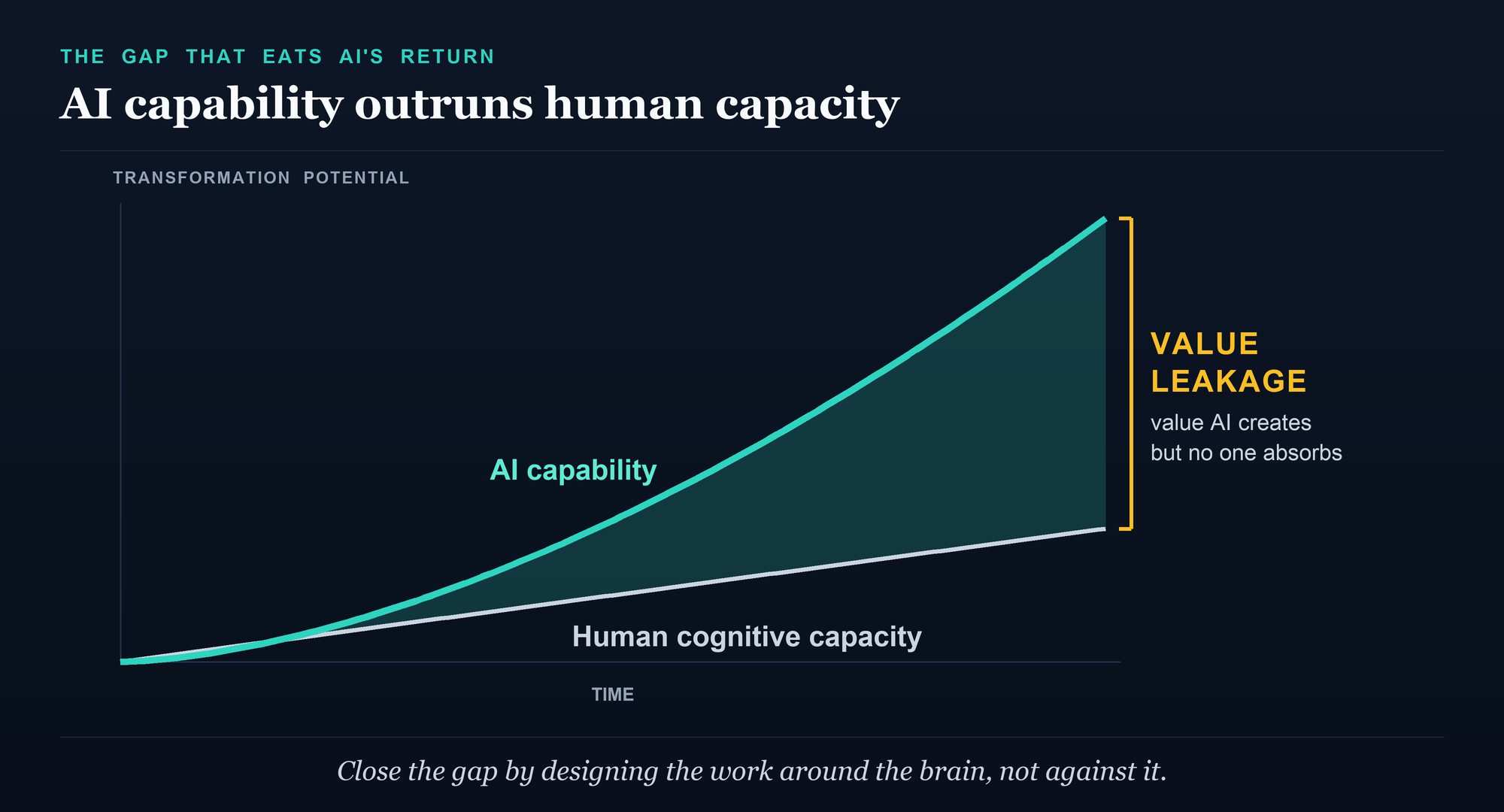
I recently sat in on a McKinsey Health Institute webinar and watched a single slide reframe the entire AI conversation for me. Not a model benchmark. Not a productivity curve. A line chart with two trajectories: artificial intelligence capability climbing steeply, and human cognitive capacity climbing slowly beside it. The widening space between the two carried a label I have not been able to stop thinking about since. Value leakage.1
The argument underneath it is deceptively simple. We have spent three years asking what AI can do. The harder question, the one that actually decides whether any of this pays off, is what the human next to the AI can still absorb. On current trajectory, the answer is less than we think, and less than we need. The bottleneck to AI value is not the technology. It is human capacity.1
That framing comes out of a new report the World Economic Forum and the McKinsey Health Institute released in January, The Human Advantage: Stronger Brains in the Age of AI. I read all thirty-three pages of it. Most of the coverage has fixed on the eye-watering economic numbers, and those numbers are real. But the report's deeper move, and the one the live panel sharpened past anything in the written text, is to name the brain itself as the strategic asset of the AI era. They call it brain capital.2
What the report actually says
Brain capital, in their definition, is two things fused together. Brain health: optimal brain functioning across the lifespan, the prevention and treatment of mental, neurological, and substance-use conditions. And brain skills: the cognitive, interpersonal, self-leadership, and technological-literacy abilities that let people adapt, relate, and contribute. Health is the foundation. Skills are what you build on it. Together they are recast not as a wellness line item but as a driver of long-term economic and social value.2
The economic case is built to hold a CFO's attention. Scaling proven brain-health interventions, the report estimates, could avert 267 million disability-adjusted life years and generate up to 6.2 trillion dollars in cumulative GDP gains by 2050. Brain-health conditions already account for roughly a quarter of the total global disease burden. Dementia in adults over 65 has risen 160 percent in three decades, from 18.7 million people in 1991 to 49 million in 2021. The World Health Organization counts about 12 billion working days lost to depression and anxiety every year, at a cost near a trillion dollars in lost productivity, while fewer than 2 percent of health budgets go to mental health. These figures measure different things and should not be stacked into one number, but they point the same direction: we have been treating the most economically important organ in the workforce as an afterthought.2,3
Then the AI overlay. Three out of four jobs will be fundamentally reshaped by AI, McKinsey's workforce research finds, and the ability to use AI tools well has grown sevenfold in two years. The World Economic Forum's own Future of Jobs survey puts it at 59 percent of workers needing significant retraining by 2030. The skills employers say they will need most for the future are, disproportionately, the ones the report classifies as brain skills: analytical thinking, resilience, creativity, curiosity, leadership. The work that is left for humans is precisely the work that depends on a healthy, well-functioning brain.2,4
The reframe nobody is making
Here is where the live session went somewhere the published report only gestures toward, and where I think the real story sits.
The consulting world has spent the past year documenting an awkward fact: most organizations are not getting the returns they expected from AI. Boston Consulting Group put a structure on it that has stuck. Of the value AI creates, they estimate that roughly 10 percent comes from the algorithms, about 20 percent from the technology and data plumbing, and a full 70 percent from people, process, and organizational change. Only a small minority of companies are capturing meaningful financial gains. The lesson almost everyone drew was that AI is a change-management problem, not a technology arms race.5
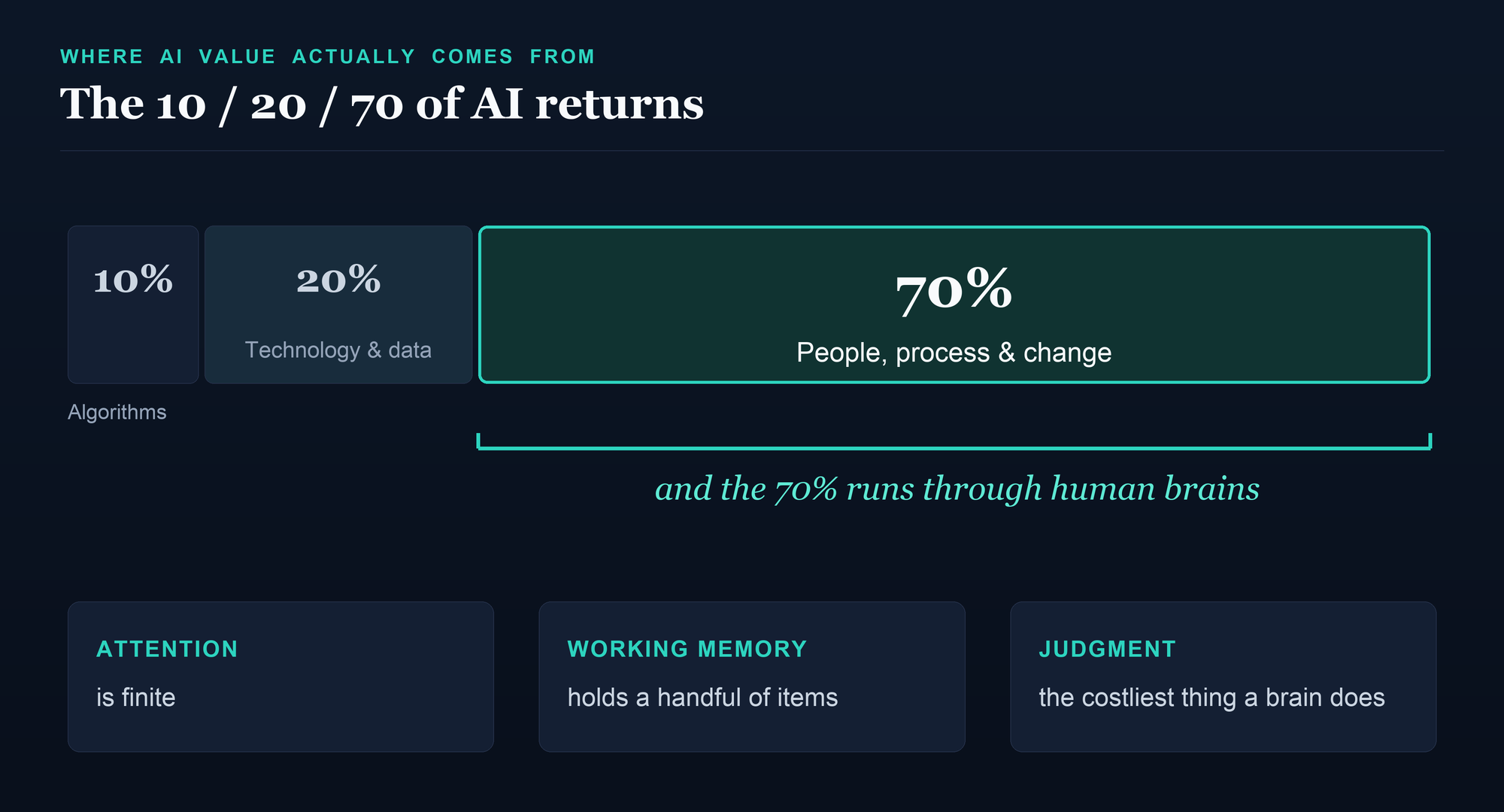
True, but incomplete. Because that 70 percent is not an abstraction about culture or workflows. It runs through actual human brains, with actual biological limits. Attention is finite. Working memory holds only about four items at a time, not the seven of folklore. Executive function degrades under stress, sleep debt, and interruption. When you hand a knowledge worker a fleet of AI tools that each generate more output to review, more decisions to make, and more context to hold, you have not removed the cognitive load. You have concentrated it. The work shifts from execution, which AI now does, to judgment, which it cannot. And judgment is the most metabolically expensive thing a brain does.6,1
Jacqueline Brassey, who directs healthy workforces and research science at the McKinsey Health Institute and sat on the launch panel, said it more plainly than the report does. The bottleneck usually isn't the technology, she told the audience. It is human capacity. Then the line I cannot shake: you can talk about it like a value leakage, where the bigger the gap between what AI can do and what people can absorb, the more of AI's potential value goes uncaptured. Her example is the one every operator should sit with. Give a customer-service team an AI that handles the routine inquiries, and the volume of work drops, but every call still standing is an escalation, a hard case, a judgment call. The easy work is gone. What is left is pure cognitive load. The headcount math looks like efficiency. The brain math looks like overload.1
That is the bridge the brain-capital frame builds and almost no one else is building. BCG's unexplained 70 percent is not only organizational. At the bottom of it is the literal cognitive capacity of overloaded people. Value leakage is what happens when AI capability outruns the brain that is supposed to direct it. You can buy more model. You cannot buy more working memory.
You can buy more model. You cannot buy more working memory. The ceiling on AI's return is the brain in the loop, and most organizations are letting it leak away.
The evidence is already arriving
This is not speculation, and the early data should give pause to anyone deploying AI at scale without a plan for the humans.
Start with the mechanism, because it has a name and a long research history. Cognitive offloading is what psychologists call shifting mental work onto an external aid to reduce the demand on your own brain. It is mostly benign and often smart: that is what a notebook, a calculator, or a calendar is for. But there is a documented cost. The classic demonstration is the so-called Google effect, where people who expect to be able to look information up later remember the information itself less, and remember only where to find it. We have been outsourcing memory to machines for years. AI moves the outsourcing up the stack, from facts to thinking.7
The most rigorous look so far at what that does to knowledge workers came this year from Microsoft Research and Carnegie Mellon, published at the CHI 2025 conference. They surveyed 319 knowledge workers about 936 real tasks they had done with AI. The finding, in the authors' own words, was that higher confidence in the AI was associated with less critical thinking, while higher confidence in oneself was associated with more. People who trusted the tool more thought less, and their outputs converged toward a narrower, more uniform set of answers. The study is self-reported, so read it as a strong signal rather than a proof, but the direction is hard to wave away.7
A widely circulated preprint from the MIT Media Lab went further, and I want to flag clearly that it is a preprint, not yet peer-reviewed, with only 54 participants. The researchers used EEG to watch the brains of people writing essays with ChatGPT, with a search engine, and with nothing but their own heads. The brain-only group showed the strongest, most distributed neural connectivity. The AI group showed the weakest. The authors coined a phrase for what they think is happening: cognitive debt. The participants who leaned hardest on the AI also had the most trouble quoting back work that had supposedly just come from them. Treat the specifics with caution, but note that it points the same way as the peer-reviewed survey.8
The learning research is firmer, and more unsettling, because it can run controlled experiments. A study of more than 600 adults found that heavier use of AI tools was associated with lower critical-thinking scores, an effect that ran through cognitive offloading and was strongest in the youngest users; the authors are careful, and so am I, that this is a correlation, not proof of cause.9 A randomized trial of university students found that ChatGPT raised the quality of the essays they turned in but produced no gain in what they actually learned or retained, a gap the researchers named metacognitive laziness: the AI quietly takes over the self-regulation that learning requires.10 The cleanest evidence is a randomized controlled trial of roughly a thousand high-school students, published in the Proceedings of the National Academy of Sciences. Students who practiced with an unguarded version of ChatGPT did better while they had it, and then scored 17 percent worse than peers who never used it once it was taken away for the exam. The crutch worked until it was removed, and then it had quietly weakened the very muscle it was assisting.11
Hold onto that study, because it also contains the way out, and I will come back to it.
Meanwhile the load is rising on its own, independent of any of this. The average knowledge worker's sustained attention on a single screen has fallen over two decades from about two and a half minutes to roughly 47 seconds, and after a real interruption it takes around 25 minutes to fully return to the original task.12 The McKinsey Health Institute's survey of more than 30,000 employees across 30 countries found that more than one in five report burnout symptoms, and that toxic workplace behavior, not individual weakness, predicts the lion's share of it. On the panel, Brassey put the live numbers higher still: one in five reporting burnout, one in two reporting high exhaustion, and in her own recent data those figures climbing to 70 or 80 percent. She has a useful reframe for it. Burnout symptoms, she argues, are really a measure of brain strain. We are pouring AI onto brains that were already at their limit.1
But doesn't AI make us smarter?
A fair reader will push back here, and should. The same period has produced some of the most encouraging productivity research in a generation, and an honest case has to hold both.
When a controlled experiment gave 453 professionals access to ChatGPT for writing tasks, it cut the time they spent by about 40 percent and raised the quality of their output by about 18 percent, and the largest gains went to the weakest writers, narrowing the gap between them and the strongest.13 A study of more than 5,000 customer-support agents found the same shape: a 14 percent productivity lift overall, and a 34 percent lift for the least experienced workers, with little effect on the experts.14 Used well, AI is a leveler. It can lift a floor faster than it lifts a ceiling.
So which is it, crutch or amplifier? The honest answer is that it depends entirely on design, and we actually have the evidence to say so. Return to that high-school trial. The same researchers tested two versions of the AI. The unguarded one became the crutch that left students worse off. But a second version, redesigned as a tutor with guardrails that prompted students to work through the reasoning rather than handing them the answer, erased the harm and produced the largest learning gains of any group. Same model. Opposite outcome. The variable was not the technology. It was whether the tool was built to make the human think or to let the human stop thinking.11
The complement to that is a study of 758 consultants that mapped what its authors called a jagged technological frontier. Inside the range of tasks AI was actually good at, the consultants using it did markedly better. Outside that range, on tasks that fell just past AI's competence, the consultants using it were about 19 percentage points more likely to get the wrong answer, because the tool produced confident, plausible, wrong output and the humans went along with it.15 The lesson of all of this is not that AI erodes the brain or that it augments it. It is that AI augments capable, rested, engaged brains operating inside its competence, and erodes tired, over-trusting brains operating outside it. Which of those two an organization gets is a function of how it designs the work. That is the whole argument for brain capital in one sentence.
What cognitive load actually means, from the clinical side
I want to slow down on the phrase cognitive load, because it gets used loosely and the biology is not loose at all. As a physician, when I hear cognitive load I hear specific, measurable things. Working memory, the mental scratchpad that holds only a handful of items you are actively manipulating. Executive function, the prefrontal machinery that plans, inhibits, and switches between tasks. Allostatic load, the cumulative wear of chronic stress on the brain and body. These are not metaphors. They degrade in predictable ways under exactly the conditions modern AI-saturated work creates: constant context-switching, decision density, and the low-grade vigilance of supervising systems you do not fully trust.
And they degrade in ways you can measure in real decisions. The most famous demonstration is a study of parole judges whose rate of favorable rulings reportedly collapsed across each session and snapped back after a food break. That study is vivid and it is also contested, so I will not lean on it, and a careful preregistered study in 2025 failed to find decision fatigue at all in a large clinical dataset. But the cleaner medical evidence is harder to dismiss. Across nearly 22,000 clinic visits, physicians prescribed more antibiotics, including clearly unnecessary ones, as the session wore on. Across more than 600,000 primary-care appointments, opioid prescribing rose from 4 percent early in the day to more than 5 percent late, with no matching rise in safer alternatives, pointing to fatigue rather than sicker patients. Appropriate cancer-screening orders fell from 64 percent at 8 a.m. to 48 percent by late afternoon. The brain that has been making consequential decisions all day is not the same instrument at hour eight that it was at hour one.16,17
This is why the two halves of brain capital cannot be separated, and why a meditation app does not fix it. You cannot train resilience or analytical thinking into a brain that is sleep-deprived, chronically stressed, and interrupted every two minutes. Brain health is the substrate. Brain skills are what that substrate can express when it is intact. The report makes the point with the science. The clinic makes it every day, with people who are not short on grit but are running an organ past its operating limits.
Why this lands hardest in healthcare
If there is a workforce where this is not theoretical, it is mine. Clinicians carry among the highest cognitive loads of any profession and post among the highest burnout rates. Physician burnout peaked at a startling 63 percent in 2021 and, after a real and welcome decline, still sat above 45 percent in 2023, well above other US workers even after adjustment.18 Much of the load is not clinical at all. For every hour a physician spends face to face with patients, studies find roughly two more hours go to the electronic health record and desk work, with another one to two hours of after-hours documentation that clinicians call pajama time. The software itself scores an F for usability, and the worse it scores, the more its users burn out.19
Now layer AI onto that. The promise of ambient AI scribes, which listen to a visit and draft the note, is real, and the early enthusiasm is understandable: large rollouts report meaningful time savings and clinicians who feel more present with patients. But the rigorous studies are more sobering, and they are the ones I would put under a physician's name. A randomized trial found one scribe vendor cut documentation time while another, tested head to head, did not move it at all. A two-year study across five hospitals found the tools saved 13 to 16 minutes a day, did not significantly reduce after-hours work, and helped mainly the heaviest users, who were a minority. The note still has to be read and corrected, because the draft contains the occasional clinically significant error, and that review is a new cognitive task that partly replaces the old one rather than removing it. The time savings, the authors concluded, were unlikely to fully explain the changes in burnout either way.20
There is a deeper trap underneath the scribe debate, and it is the one the brain-capital lens sees most clearly. Supervising an AI is itself cognitively expensive. The literature on automation bias shows that the harder an AI's output is to verify, the more we over-trust it, precisely because verification is effortful and the tired brain takes the path of least resistance. In one striking study, radiologists shown a confidently wrong AI reading saw their own accuracy collapse, the inexperienced ones from about 80 percent to 20 percent. The engineer Lisanne Bainbridge named this the irony of automation back in 1983: automate the easy parts and you leave the human with the exhausting job of vigilant monitoring, and the more reliable the automation, the less able the human becomes to catch the moment it fails. We are about to run that experiment across every clinic and call center in the country.21
I have spent the last stretch of my own work at the narrow end of this problem. Brain Revives is not brain health in general. It is the post-discharge window after traumatic brain injury, the first 90 days home, the part of recovery the system funds least and patients survive worst. Sitting in a brain-capital webinar built for CEOs and CFOs, I kept hearing the same truth from the opposite end of the telescope. Whether it is a patient relearning to hold a thought after a brain injury or a knowledge worker trying to keep four things in mind while an AI generates a fifth, the binding constraint is the same organ, and we have spent a generation pretending it has no limits.
The other half: brain health is buildable
It would be easy to read all of this as fatalism, as if the brain were a fixed tank we are draining. It is not. The most important thing the report gets right is that brain capital is an asset you can invest in and grow, and the prevention evidence that has matured in the last two years is genuinely good news.
The headline result came in 2025 from the US POINTER trial, the largest American test of its kind: more than 2,000 older adults at risk for decline, randomized for two years to either a structured program of exercise, the MIND diet, cognitive training, and regular blood-pressure monitoring, or a lighter self-guided version. The structured group measurably outperformed on global cognition. Both groups improved, so the honest read is that structure beats good intentions, not that lifestyle beats nothing. But it confirms what the earlier Finnish FINGER trial first showed: a multidomain lifestyle intervention can move the cognitive trajectory of an aging brain, and that finding is now being replicated across more than 40 countries.22,23
The prevention numbers are striking when you sit with them. The Lancet Commission on dementia concluded in its 2024 update that nearly half of dementia cases, about 45 percent, are potentially preventable or delayable by addressing 14 modifiable risk factors across the lifespan, from education and hearing loss to hypertension, LDL cholesterol, and air pollution. Roughly 84 percent of the global burden of stroke traces to modifiable risk. And a simple 21-point brain-care score built at Mass General Brigham found that every five-point improvement was associated with a 43 percent lower risk of cardiovascular disease and a third lower risk of late-life depression.24,25,26
That is exactly why the economic framing is not just rhetoric. The returns on building brain capital early are among the highest in all of economics, with high-quality early-childhood programs returning up to 13 percent a year, and employers see roughly four to five dollars back for every dollar spent on workplace mental health. The McKinsey and WEF modeling that investing in employee health could add as much as 12 percent to global GDP is a projection, not a measured result, but it sits on top of a real and growing evidence base that the brain pays back what you put into it.27
The part employers can actually do something about
The most useful thing in the live session was not a statistic. It was a short list of design principles for what the panel called AI-powered workplaces, built around brain capital instead of bolting wellness onto a broken system. The framing is worth taking wholesale. Calibrate cognitive load: deliberately match the demands of a role to what a human brain can sustain, rather than treating capacity as infinite. Protect cognitive capacity: defend focus, recovery, and sleep the way an athletic program defends physical recovery. Enable focus, so people can exercise the good judgment that is now the scarce input. Build adaptive brain skills, upgrading how people think and learn rather than only which tools they use. And design brain-positive environments across the social, physical, and digital surfaces of work.1
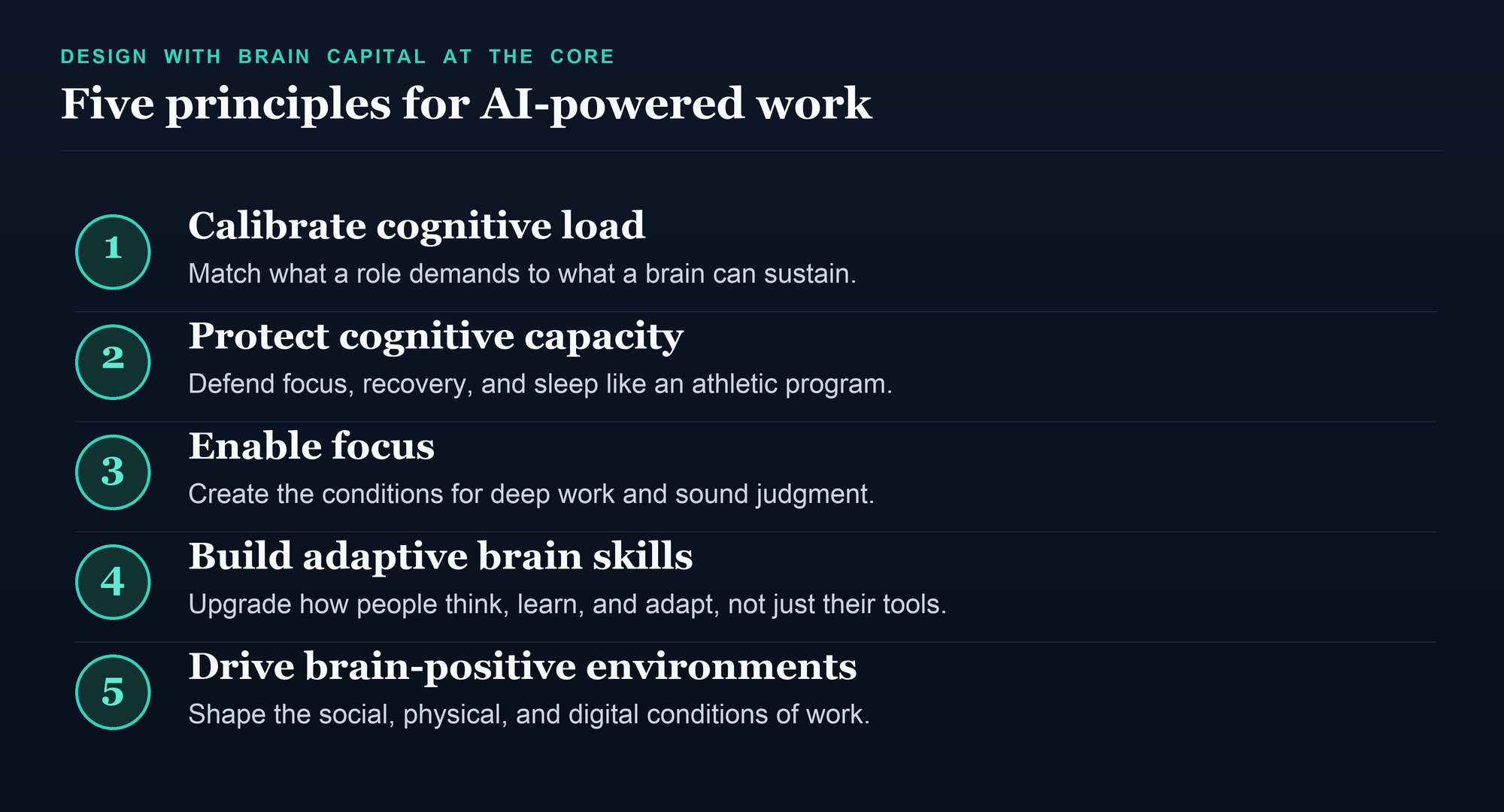
Brassey's own starting point is blunter: measure first. Track exhaustion and what she calls the AI energy of the organization the way you would track any other operating metric, find the hotspots, and design around them. And calibrate cuts both ways. The discipline is not only to stop overloading people, but, once AI clears the routine work, not to underload them into boredom either. The point is to architect the load, not to assume the technology will balance it for you.1
None of this is soft, and the guardrail evidence tells you why it works. Remember the high-school trial: the version of the AI that forced engagement built capability, and the version that allowed disengagement destroyed it. A brain-positive workplace is the organizational version of that guardrail. There is already an operator literature to draw on. The Center for BrainHealth at the University of Texas at Dallas runs a measurable workplace program, and the Business Collaborative for Brain Health has published a unified model of the risk and resilience factors, sleep, stress, and social connection, that cut across mental health, neurological health, and workplace performance. The scaffolding for treating the brain as an asset to be managed, rather than a resource to be spent, already exists. What is missing is operators willing to run it.28
Brain capital is a strategy, not a perk
The reason this report matters, and the reason I think the value-leakage frame outlives the Davos news cycle, is that it moves the brain out of the wellness budget and into the strategy deck. For most of my career, anything touching mental or cognitive health in the workplace was filed under benefits: nice to have, first to be cut. Erica Coe, the Health Institute's global executive director, drew the line cleanly as the panel closed. For decades we invested in physical capital, then financial capital, then digital capital. In the age of AI, she argued, the most valuable and most underinvested resource left may be brain capital. The deliberate word in the phrase is the second one. The argument now on the table is that in an AI economy, the health and skill of your people's brains is the rate-limiting input to everything the technology is supposed to deliver. That is not an HR initiative. That is a CEO-and-board question, which is exactly where the report says it belongs.1,2
The companies that win the next decade will not be the ones with the most model access. Everyone will have that. They will be the ones who treated human cognitive capacity as the scarce, defensible, investable asset it actually is, and built the work around the brain instead of against it. The bottleneck was never the machine. It was always us. The only question is whether we design for that, or keep letting the value leak out through the gap.
Disclosure: NewsHX has no commercial relationship with the World Economic Forum, the McKinsey Health Institute, Boston Consulting Group, the Center for BrainHealth, or the Business Collaborative for Brain Health. These organizations are named as sources, not endorsements.
Deploying AI across a workforce that is already at its cognitive limit?
The hard part of an AI rollout is not the model. It is the human capacity it lands on. A3HCS brings a physician-executive lens to designing work around the brain instead of against it: cognitive-load calibration, brain-positive workplace design, and the operating discipline to turn a wellness line item into a strategic capability.
Start the conversation at A3HCS.orgReferences
- McKinsey Live webinar, “Brain health: Helping individuals, organizations, and societies thrive in the age of AI,” featuring Erica Coe, Kana Enomoto, and Jacqueline Brassey; hosted by Lucia Rahilly. McKinsey Health Institute, June 25, 2026. Replay at mckinsey.com/live.
- World Economic Forum and McKinsey Health Institute. The Human Advantage: Stronger Brains in the Age of AI. Insight Report, January 2026.
- World Health Organization. “Mental health at work,” fact sheet, updated September 2024 (12 billion working days, ~US$1 trillion lost productivity); WHO Mental Health Atlas (under 2 percent of health budgets).
- World Economic Forum, The Future of Jobs Report 2025 (59 percent of workers need reskilling by 2030). The “three of four jobs” and “sevenfold in two years” figures are from McKinsey Global Institute, “Agents, robots, and us: Skill partnerships in the age of AI,” November 2025.
- Boston Consulting Group. From Potential to Profit: Closing the AI Impact Gap (the 10-20-70 principle: ~10 percent algorithms, 20 percent technology and data, 70 percent people, process, and change; only ~5 percent of firms capturing substantial gains). 2025.
- Working-memory capacity: Cowan N, “The magical number 4 in short-term memory,” Behavioral and Brain Sciences 2001;24(1):87-114; cf. Miller GA, Psychological Review 1956;63(2):81-97.
- Cognitive offloading and critical thinking: Risko EF, Gilbert SJ, “Cognitive Offloading,” Trends in Cognitive Sciences 2016;20(9):676; Sparrow B, Liu J, Wegner DM, “Google Effects on Memory,” Science 2011;333:776; Lee H-P, et al., “The Impact of Generative AI on Critical Thinking,” Microsoft Research and Carnegie Mellon University, CHI 2025 (319 knowledge workers, 936 tasks).
- Kosmyna N, et al. “Your Brain on ChatGPT: Accumulation of Cognitive Debt When Using an AI Assistant for Essay Writing Task.” MIT Media Lab. arXiv preprint 2506.08872, June 2025 (N=54). Preprint, not yet peer-reviewed.
- Gerlich M. “AI Tools in Society: Impacts on Cognitive Offloading and the Future of Critical Thinking.” Societies 2025;15(1):6 (n=666; correlational).
- Fan Y, et al. “Beware of metacognitive laziness: Effects of generative artificial intelligence on learning motivation, processes, and performance.” British Journal of Educational Technology 2025;56(2):489-530.
- Bastani H, et al. “Generative AI without guardrails can harm learning: Evidence from high school mathematics.” PNAS 2025;122(26):e2422633122.
- Attention and interruption: Mark G, Attention Span (Hanover Square Press, 2023); Mark G, Gonzalez VM, Harris J, “No Task Left Behind? Examining the Nature of Fragmented Work,” Proc. CHI 2005 (~25-minute recovery after interruption).
- Noy S, Zhang W. “Experimental evidence on the productivity effects of generative artificial intelligence.” Science 2023;381(6654):187-192 (n=453).
- Brynjolfsson E, Li D, Raymond L. “Generative AI at Work.” Quarterly Journal of Economics 2025;140(2):889-942 (5,179 support agents).
- Dell'Acqua F, et al. “Navigating the Jagged Technological Frontier.” Harvard Business School Working Paper 24-013, 2023 (758 consultants). Working paper.
- Decision fatigue, with caveats: Danziger S, Levav J, Avnaim-Pesso L, “Extraneous factors in judicial decisions,” PNAS 2011;108(17):6889 (vivid but contested; see Weinshall-Margel & Shapard, PNAS 2011, and Glockner, Judgment and Decision Making 2016; a preregistered null result is Andersson D, et al., Communications Psychology 2025;3(1):33).
- Clinical decision fatigue: Linder JA, et al., “Time of Day and the Decision to Prescribe Antibiotics,” JAMA Internal Medicine 2014;174(12):2029 (21,867 visits); Neprash HT, Barnett ML, JAMA Network Open 2019;2(8):e1910373 (678,319 appointments); Hsiang EY, et al., JAMA Network Open 2019;2(5):e193403 (cancer-screening orders).
- Shanafelt TD, et al. Physician burnout series: Mayo Clinic Proceedings 2022;97(12):2248 (62.8 percent peak, 2021) and 2025;100(7):1142 (45.2 percent, 2023).
- EHR and documentation burden: Sinsky C, et al., “Allocation of Physician Time in Ambulatory Practice,” Annals of Internal Medicine 2016;165(11):753 (the 2-to-1 ratio); Arndt BG, et al., “Tethered to the EHR,” Annals of Family Medicine 2017;15(5):419 (5.9 EHR hours/day, 1.4 after-hours); Melnick ER, et al., Mayo Clinic Proceedings 2020;95(3):476 (EHR usability “F”).
- AI scribe evidence: Rotenstein L, et al., ambient-AI-scribe study across five hospitals, JAMA 2026 (13-16 min/day saved, no significant after-hours reduction); Lukac S, et al., randomized trial, NEJM AI 2025;2(12) (vendor-dependent results); Tierney AA, et al., “Ambient Artificial Intelligence Scribes,” NEJM Catalyst 2024;5(3) (3,442 physicians; output framed as a draft for physician editing).
- Automation bias and the cost of supervising AI: Lyell D, Coiera E, “Automation bias and verification complexity,” JAMIA 2017;24(2):423; Dratsch T, et al., “Automation Bias in Mammography,” Radiology 2023;307(4):e222176 (simulated wrong AI); Bainbridge L, “Ironies of Automation,” Automatica 1983;19(6):775.
- Baker LD, et al. “Structured vs Self-Guided Multidomain Lifestyle Interventions for Global Cognitive Function: The US POINTER Randomized Clinical Trial.” JAMA, July 28, 2025; doi:10.1001/jama.2025.12923 (N=2,111).
- Ngandu T, et al. “A 2 year multidomain intervention (FINGER): a randomised controlled trial.” Lancet 2015;385(9984):2255-2263; Worldwide FINGERS network (40+ countries).
- Livingston G, et al. “Dementia prevention, intervention, and care: 2024 report of the Lancet Standing Commission.” Lancet 2024;404(10452):572-628 (~45 percent of cases preventable; 14 risk factors).
- GBD 2021 Stroke Risk Factor Collaborators. “Global, regional, and national burden of stroke and its risk factors, 1990-2021.” Lancet Neurology 2024;23(10):973-1003 (~84 percent of stroke burden attributable to modifiable risk).
- McCance Brain Care Score: Senff J, Singh SD, et al., Family Practice 2025 (5-point higher score, 43 percent lower cardiovascular risk; UK Biobank, n=416,370); Singh SD, et al., Frontiers in Psychiatry 2024 (33 percent lower late-life depression).
- ROI: Heckman early-childhood return (up to 13 percent/year); Deloitte UK, Mental health and employers (2024) (~£4.70 per £1); McKinsey Health Institute and World Economic Forum, Thriving Workplaces (2025) (up to 12 percent of global GDP, modeled potential).
- Operator frameworks: Center for BrainHealth (University of Texas at Dallas), BrainHealthy Workplace program; Business Collaborative for Brain Health (UsAgainstAlzheimer's), unified model of brain-health risk and resilience factors.