
Every few months a market report announces that the migraine space is being transformed, and the headline number gets bigger. The therapeutic class count climbs. The forecast revenue climbs. The pipeline slide gets more crowded. All of it is true, and almost none of it answers the question that actually matters to a person with migraine: will I get my life back.
I want to argue something that runs against the celebratory framing. The last decade did something genuinely historic. It solved the molecule problem in migraine. We now have preventive therapies built on the actual biology of the disease, and they work. But the data from real-world use, and the most recent guidance from the field's own leadership, point to a harder and less marketable truth. The unsolved problem in migraine is no longer whether we can prevent attacks. It is whether we can get patients all the way to freedom, keep them on the therapy that gets them there, and pay for it. That is the decade ahead, and it will be won on residual burden, persistence, and access, not on chemistry.
Start with the burden, stated honestly
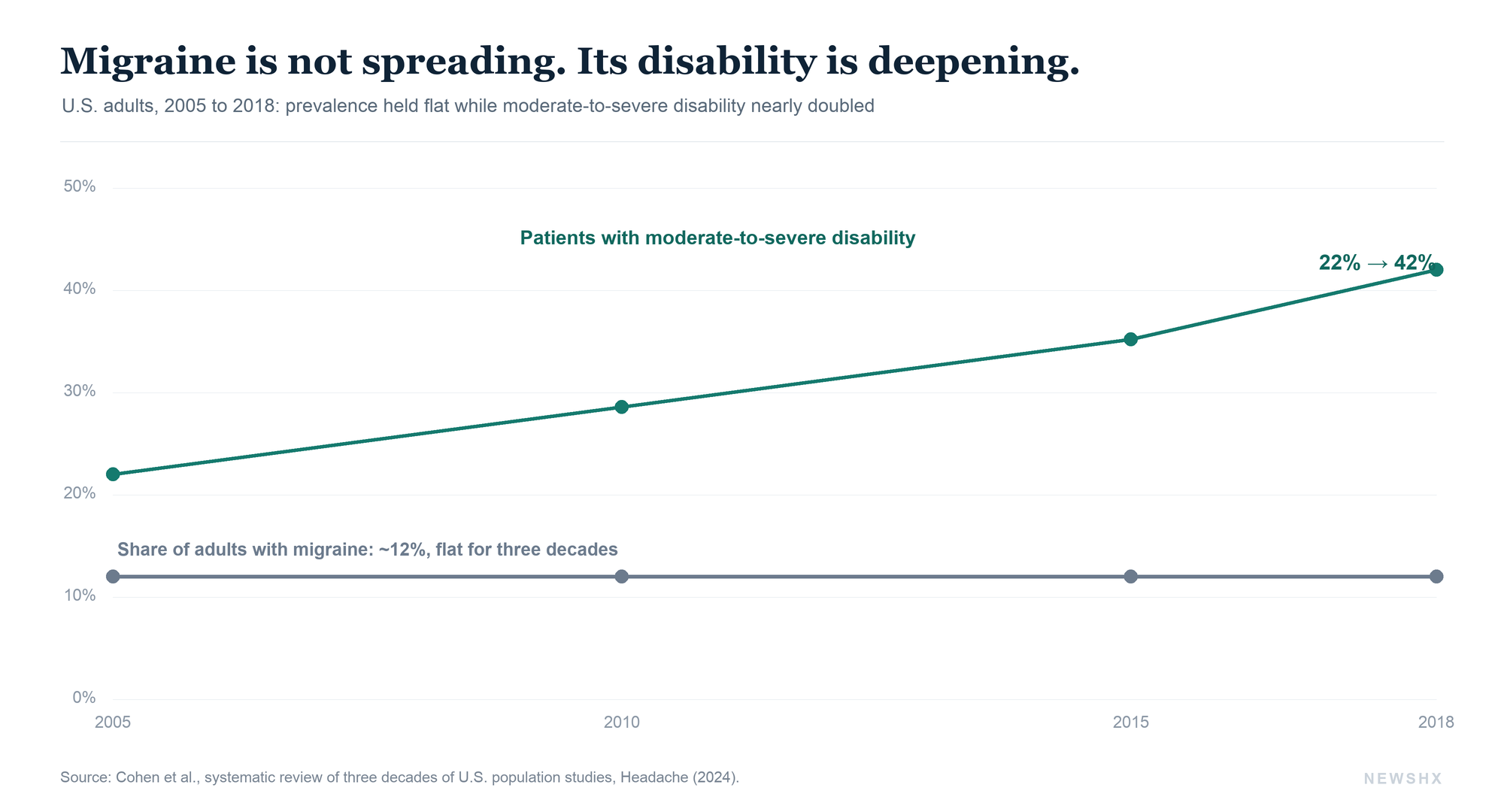
Migraine is not a nuisance headache, and the epidemiology has been stable long enough that we should stop being surprised by it. A 2024 systematic review of three decades of U.S. population studies put migraine prevalence at roughly 12 percent overall, between 11.7 and 14.7 percent across studies, with women at 17 to 19 percent and men at 6 to 7 percent.1 Chronic migraine, defined as 15 or more headache days a month, affects close to 1 percent of adults.1 Globally, the Global Burden of Disease analysis ranks migraine as the second-leading cause of years lived with disability, and the leading cause among women.2
Here is the number that should reframe the conversation. Over those same three decades, while prevalence stayed flat, the share of people with migraine carrying moderate-to-severe disability rose, from 22 percent in 2005 to roughly 42 percent in 2018 by the standard disability measure.1 The disease is not spreading. The disability it produces is deepening, or we are finally measuring it honestly. Either way, the burden is concentrated in working-age adults, disproportionately women, and roughly 2.5 percent of people with episodic migraine progress to the chronic form each year.3
By the numbers. Roughly 12 percent of U.S. adults have migraine, a rate stable for three decades. Only about 31 percent of patients remain on a CGRP antibody at six months. And the field's new benchmark for being well is fewer than four migraine days a month, not a 50 percent reduction.1,9,10
That is the demand side. It is enormous, it is stable, and it is not the part we have failed to address with drugs.
The decade that solved the molecule
For most of modern medicine, migraine prevention meant borrowing drugs designed for something else, beta-blockers, antiepileptics, antidepressants, and hoping. The first dedicated chronic-migraine preventive was onabotulinumtoxinA, whose pivotal PREEMPT program showed a reduction of 8.4 headache days per month versus 6.6 on placebo.4 Real, durable, and still in use, but a modest signal and a procedure-based one.
Then the field got the biology. Calcitonin gene-related peptide turned out to be central to migraine attacks, and the therapeutics followed fast. Monoclonal antibodies against the CGRP pathway, erenumab, fremanezumab, galcanezumab, eptinezumab, and then the oral small-molecule gepants, rimegepant and atogepant, were built to target the mechanism directly. The trial data are consistent and, for migraine, remarkable. Galcanezumab cut monthly migraine days by about 4.2 to 4.3 versus 2.3 on placebo.5 Atogepant at its 60 mg dose reduced migraine days by 4.2 versus 2.5 on placebo.6 Oral rimegepant, dosed every other day, reduced days by 4.3 versus 3.5.7 Across the class, roughly half of patients hit the benchmark of a 50 percent or greater reduction, and a network meta-analysis of nineteen randomized trials found the antibodies and gepants to be safe and well tolerated, with serious adverse events no different from placebo.8
That is what a solved molecule problem looks like. We can prevent migraine, mechanistically, in a large fraction of patients, with a tolerability profile most chronic-disease drugs would envy. If the only question were whether an effective preventive exists, the answer is settled.
A faster molecule was never the bottleneck. We learned to prevent migraine on purpose. The next decade is no longer about that.
Where the story stops being a success story
Now look at what happens after the prescription is written, because this is where the celebratory framing breaks.
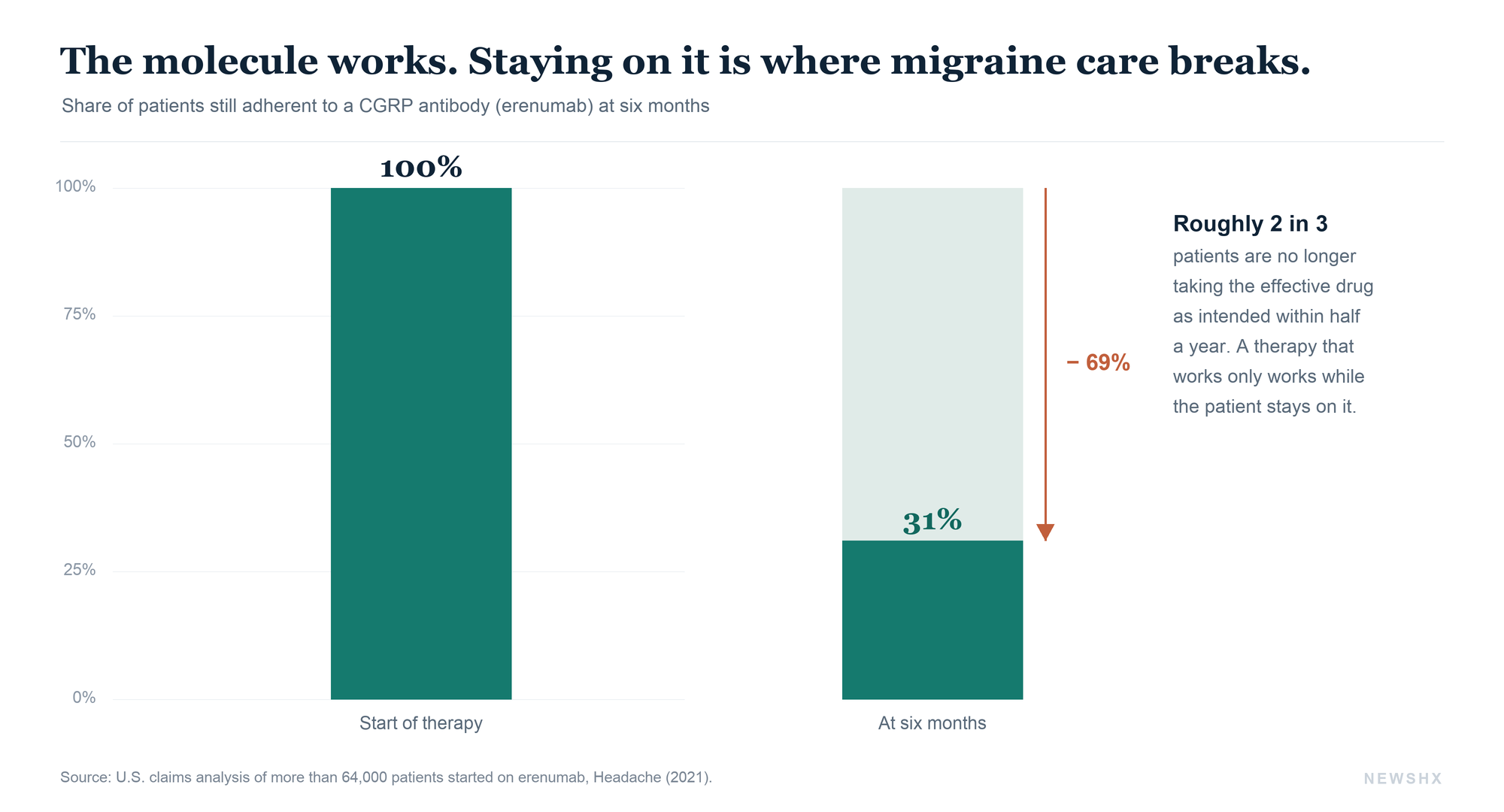
In a U.S. claims study of more than 64,000 patients started on erenumab, only about 31 percent were adherent at the standard threshold over the following six months.9 Adherence was better than the old oral preventives, a low bar, but the majority of patients were not taking the effective drug as intended within half a year. A therapy that works in the trial does nothing for a patient who is no longer on it. The molecule was never the failure point. The persistence was.
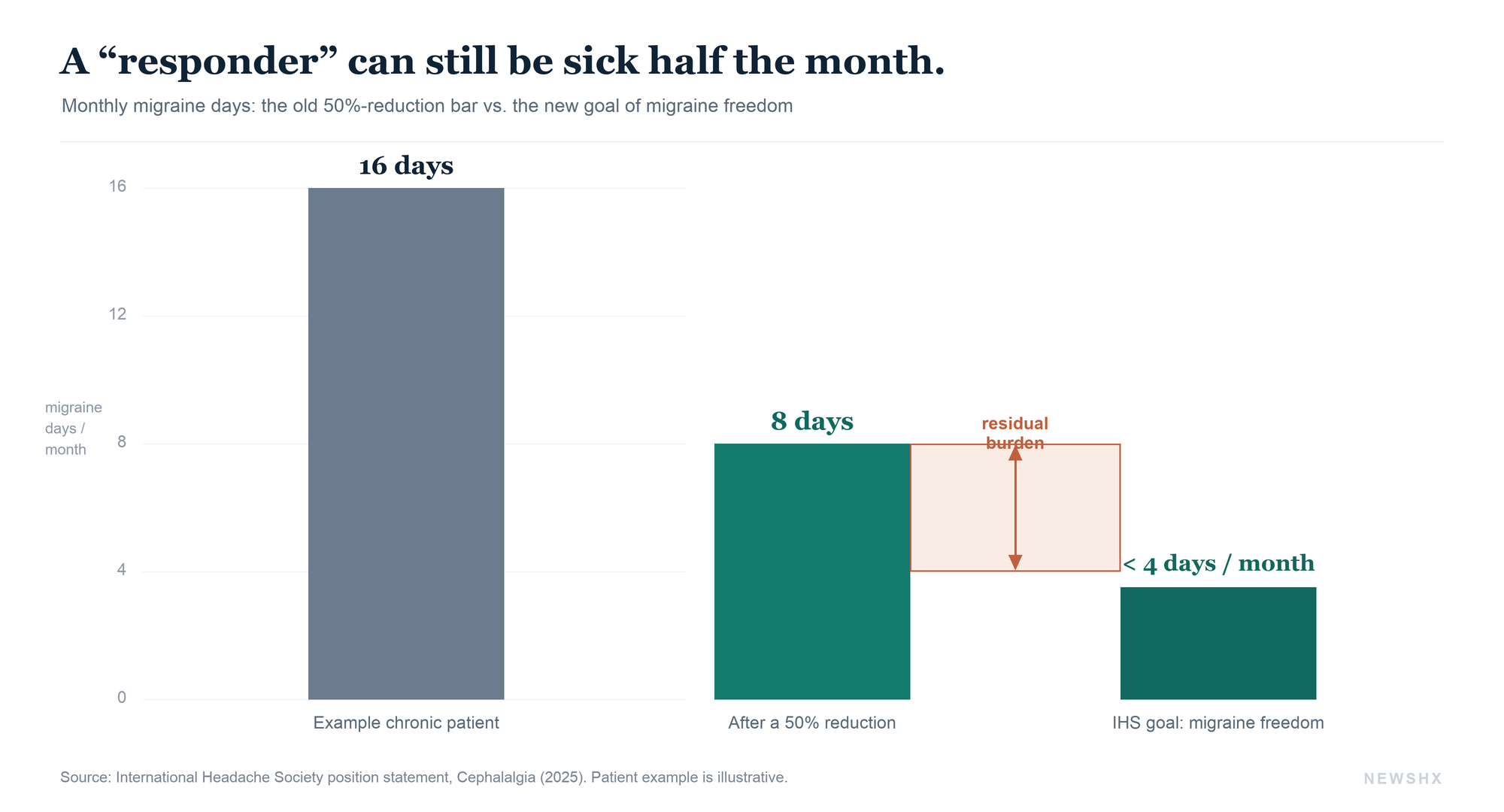
And even among patients who stay on therapy and respond, response turns out to be a generous word. In early 2025, the International Headache Society issued a position statement with an uncomfortable thesis: a 50 percent reduction in migraine days, the figure the entire field has used to declare success, may not fully restore quality of life.10 A patient who goes from sixteen migraine days a month to eight is a trial responder and is still sick half the month. The IHS argued for abandoning percentage-based success in favor of absolute goals, migraine freedom or fewer than four migraine days a month, and for treating residual burden as the thing that still needs solving.10 That is the headache field's own leadership saying, in effect, that clearing the bar we set is not the same as getting patients well.
This is the real frontier, and it is not a chemistry problem. It is a problem of getting the right patient onto the right therapy, keeping them there, escalating when residual burden persists, and removing the friction that knocks people off treatment. Most of that friction, in the United States, is access.
The access reality nobody puts on the pipeline slide
The CGRP therapies arrived into a payer system designed to slow their use. Step-therapy protocols routinely require patients to fail two or more older oral preventives before a plan will cover an antibody or gepant. Prior authorization is near-universal for these agents. The result is a structural gap between the patient a trial enrolled and the patient a formulary actually reaches, and it falls hardest on exactly the working-age, disproportionately female population carrying the most disability.
This is why two products with identical mechanisms can post different real-world results, and why the next molecule, however elegant, does not by itself move the national numbers. The binding constraint has shifted downstream of the laboratory. A pipeline measured in new mechanisms is answering a question the field has mostly already answered. The questions left are who gets access, how fast, and for how long.
A faster denial is still a denial, and a covered drug a patient cannot start is not a treatment. We solved the molecule. The gap that remains is administrative, and it is measured in weeks a patient stays sick.
What this looks like when it is your patient
I spend much of my clinical attention on the brain after it has been injured, and migraine is where that work and this story meet. Post-traumatic headache is one of the most common sequelae of traumatic brain injury, and in a large share of patients it does not present as some exotic new disorder. It presents as migraine. The Lancet Neurology review of post-traumatic headache is explicit that clinicians, lacking dedicated therapies, treat it according to its primary headache phenotype, and that phenotype is most often migraine.11 The preclinical and clinical comparisons go further: persistent post-traumatic headache and migraine are frequently indistinguishable at the bedside, and the migraine playbook is what works.12
So picture the patient I actually see. A person months out from a concussion, in the time-limited window when the brain is most able to reorganize and recover, derailed by headaches that meet every criterion for migraine. The effective preventives exist. The evidence that they help this patient exists. And the thing standing between the two is rarely the science. It is a step-therapy requirement to fail older drugs first, a prior-authorization queue, a co-pay, a refill that never happens. Every week lost in that gap is a week subtracted from a recovery window that does not reopen. The molecule is ready. The system around it is not.
So what is the pipeline actually for
None of this makes the pipeline pointless. It reframes what we should want from it. More mechanisms matter most for the patients the current classes leave behind, the ones who do not respond to CGRP blockade, or who respond only partway and live in the residual burden the IHS just named.
The most scientifically interesting candidate is the first preventive aimed at a genuinely different target: PACAP, a signaling peptide that sits parallel to CGRP in migraine biology. In a phase 2 trial published in the New England Journal of Medicine, a single infusion of the anti-PACAP antibody Lu AG09222, now bocunebart, cut migraine days by 6.2 versus 4.2 on placebo, in patients for whom two to four prior preventives had already failed.13 That last detail is the point. A new target earns its place by working where the existing targets do not. Lundbeck's PROCEED program is advancing, with a pivotal phase 3 expected to begin in the second half of 2026.14
The acute side is filling in too. In 2025 the FDA cleared Symbravo, a co-formulation of meloxicam and rizatriptan,15 and Atzumi, a dihydroergotamine nasal powder,16 both for acute treatment, meaningful for patients who tolerate or respond poorly to standard triptans. And in a first for the category, a prescription digital therapeutic, CT-132, was authorized for migraine prevention,17 a signal that non-pharmacological tools are entering the same evidentiary conversation. Even there, the head-to-head data are maturing rather than settled. The first direct comparison of two CGRP agents found galcanezumab no better than rimegepant, with both simply effective.18 The class is deep enough now that the interesting questions are about sequencing and matching, not existence.
What operators should do now
If you run a service line, a specialty practice, or a population, the implication is not to wait for the next approval. The therapeutic toolbox you need already exists. Three moves matter more than any pipeline bet.
First, measure the right endpoint. Stop reporting migraine programs on responder rate alone and start tracking residual migraine days and the share of patients reaching the IHS thresholds of optimal control or freedom. A 50 percent line on a dashboard hides patients who are still sick half the month, and what you do not measure you will not fix.
Second, treat persistence as a clinical outcome, not a pharmacy statistic. A 31 percent six-month adherence figure is an operational failure with a clinical cost. Build the follow-up touchpoints, the refill prompts, and the early-switch logic that keep responders on therapy, because the most cost-effective migraine drug is the one a patient does not abandon.
Third, work the access pathway deliberately. Map your dominant payers' step-therapy and prior-authorization rules for CGRP agents, pre-build the documentation, and route post-TBI and high-disability patients through the fastest compliant path. The gap between an effective drug and a covered drug is administrative, which means it is yours to close.
The decade's real question
If I were briefing a room of clinicians, payers, or developers on where migraine goes from here, I would tell them to stop counting molecules. The molecule problem is, to a first approximation, solved. The disease that remains is a disease of gaps, between the trial response and the restored life, between the prescription and the refill, between the labeled indication and the covered patient.
The organizations that win the next decade in migraine will not be the ones with the longest pipeline slide. They will be the ones who treat residual burden as the real endpoint, persistence as a clinical outcome rather than an afterthought, and access as part of the therapy rather than an obstacle to it. We learned how to prevent migraine. Now we have to learn how to actually deliver it.
Disclosure. NewsHX has no commercial relationship with any company or product named in this article. Market-sizing context was informed by DelveInsight's 2026 Migraine Market report; every clinical and epidemiologic claim is independently sourced to the peer-reviewed literature cited below.
Closing the gap between an effective therapy and a treated patient.
The migraine toolbox already works. The gap is operational: residual burden that responder-rate dashboards hide, persistence that collapses by month six, and access pathways that lose high-disability patients in prior authorization. A3HCS helps health systems and specialty practices turn a strong formulary into real outcomes, with a physician-executive read on measurement, adherence, and access.
Start the conversation at A3HCS.orgReferences
- Cohen F, Brooks CV, Sun D, et al. “Prevalence and burden of migraine in the United States: A systematic review.” Headache. 2024;64(5):516–532. doi.org/10.1111/head.14709
- GBD 2016 Disease and Injury Incidence and Prevalence Collaborators. “Global, regional, and national incidence, prevalence, and years lived with disability for 328 diseases and injuries, 1990–2016.” Lancet. 2017;390(10100):1211–1259. doi.org/10.1016/S0140-6736(17)32154-2
- Burch RC, Buse DC, Lipton RB. “Migraine: Epidemiology, Burden, and Comorbidity.” Neurologic Clinics. 2019;37(4):631–649. doi.org/10.1016/j.ncl.2019.06.001
- Dodick DW, Turkel CC, DeGryse RE, et al. “OnabotulinumtoxinA for treatment of chronic migraine: pooled results from the double-blind, randomized, placebo-controlled phases of the PREEMPT clinical program.” Headache. 2010;50(6):921–936. doi.org/10.1111/j.1526-4610.2010.01678.x
- Skljarevski V, Matharu M, Millen BA, et al. “Efficacy and safety of galcanezumab for the prevention of episodic migraine: EVOLVE-2.” Cephalalgia. 2018;38(8):1442–1454. doi.org/10.1177/0333102418779543
- Ailani J, Lipton RB, Goadsby PJ, et al. “Atogepant for the Preventive Treatment of Migraine (ADVANCE).” New England Journal of Medicine. 2021;385(8):695–706. doi.org/10.1056/NEJMoa2035908
- Croop R, Lipton RB, Kudrow D, et al. “Oral rimegepant for preventive treatment of migraine: a phase 2/3, randomised, double-blind, placebo-controlled trial.” Lancet. 2020;397(10268):51–60. doi.org/10.1016/S0140-6736(20)32544-7
- Messina R, Huessler EM, Puledda F, et al. “Safety and tolerability of monoclonal antibodies targeting the CGRP pathway and gepants in migraine prevention: a systematic review and network meta-analysis.” Cephalalgia. 2023;43(3). doi.org/10.1177/03331024231152169
- Hines DM, Shah S, Multani JK, et al. “Erenumab patient characteristics, medication adherence, and treatment patterns in the United States.” Headache. 2021;61(4):590–602. doi.org/10.1111/head.14068
- Sacco S, Ashina M, Diener HC, et al. “Setting higher standards for migraine prevention: A position statement of the International Headache Society.” Cephalalgia. 2025;45(2). doi.org/10.1177/03331024251320608
- Ashina H, Eigenbrodt AK, Seifert T, et al. “Post-traumatic headache attributed to traumatic brain injury: classification, clinical characteristics, and treatment.” Lancet Neurology. 2021;20(6):460–469. doi.org/10.1016/S1474-4422(21)00094-6
- Capi M, Pomes LM, Andolina G, et al. “Persistent Post-Traumatic Headache and Migraine: Pre-Clinical Comparisons.” International Journal of Environmental Research and Public Health. 2020;17(7):2585. doi.org/10.3390/ijerph17072585
- Ashina M, Phul R, Khodaie M, Löf E, Florea I. “A Monoclonal Antibody to PACAP for Migraine Prevention (HOPE).” New England Journal of Medicine. 2024;391(9):800–809. doi.org/10.1056/NEJMoa2314577
- H. Lundbeck A/S. “Positive Phase IIb data for bocunebart (Lu AG09222, anti-PACAP) in migraine prevention; pivotal Phase III planned for the second half of 2026.” PROCEED program update, 2025–2026. pharmaphorum.com/news/lundbeck-preps-phase-3-migraine-prevention-drug
- Axsome Therapeutics. “FDA approval of SYMBRAVO (meloxicam and rizatriptan) for the acute treatment of migraine, January 2025.” neurologylive.com
- Satsuma Pharmaceuticals / Shin Nippon Biomedical Laboratories. “FDA approval of ATZUMI (dihydroergotamine nasal powder) for acute migraine, April 2025.” healio.com
- Click Therapeutics. “CT-132 authorized as the first prescription digital therapeutic for migraine prevention, 2025.” neurologylive.com
- Schwedt TJ, Myers Oakes TM, Martinez JM, et al. “Comparing the Efficacy and Safety of Galcanezumab Versus Rimegepant for Prevention of Episodic Migraine.” Neurology and Therapy. 2023;13(1):85–105. doi.org/10.1007/s40120-023-00562-w