

Every hospital in America runs on people who are awake when their bodies are built to sleep. Nurses, intensivists, emergency physicians, lab techs, radiology, security, environmental services. We have decided, correctly, that this work cannot stop at sundown. What we have not done honestly is account for what it costs the people who do it.
The accounting we use today is the shift differential. Two to five dollars an hour, sometimes structured as ten to eighteen percent over base pay.1 For a registered nurse earning $35 an hour, that is roughly $3.50 to $5.25 more per hour, about $140 to $210 across a 40-hour night-shift week.1 It feels like a fair trade because it is paid in the same currency as the work. But the bill the night shift runs up is not paid in dollars. It is paid in cardiovascular disease, in years of life, and most of all in mental health. And on that ledger, the differential does not come close.
I have read enough discharge summaries and sat in enough team conferences to know that the people who staff the worst hours are the ones we can least afford to lose. So it is worth being precise about what the science actually shows, because most leaders are still treating this as a comfort issue when it is a clinical one.
What the night does to the body
Humans are diurnal. Almost every system we have, hormone release, core temperature, glucose handling, immune signaling, cell repair, is timed by a master clock that expects light by day and dark by night. Night shift work does not just make people tired. It forces those systems to run out of phase with one another, a state researchers call circadian disruption. The downstream effects are now well documented across large populations.
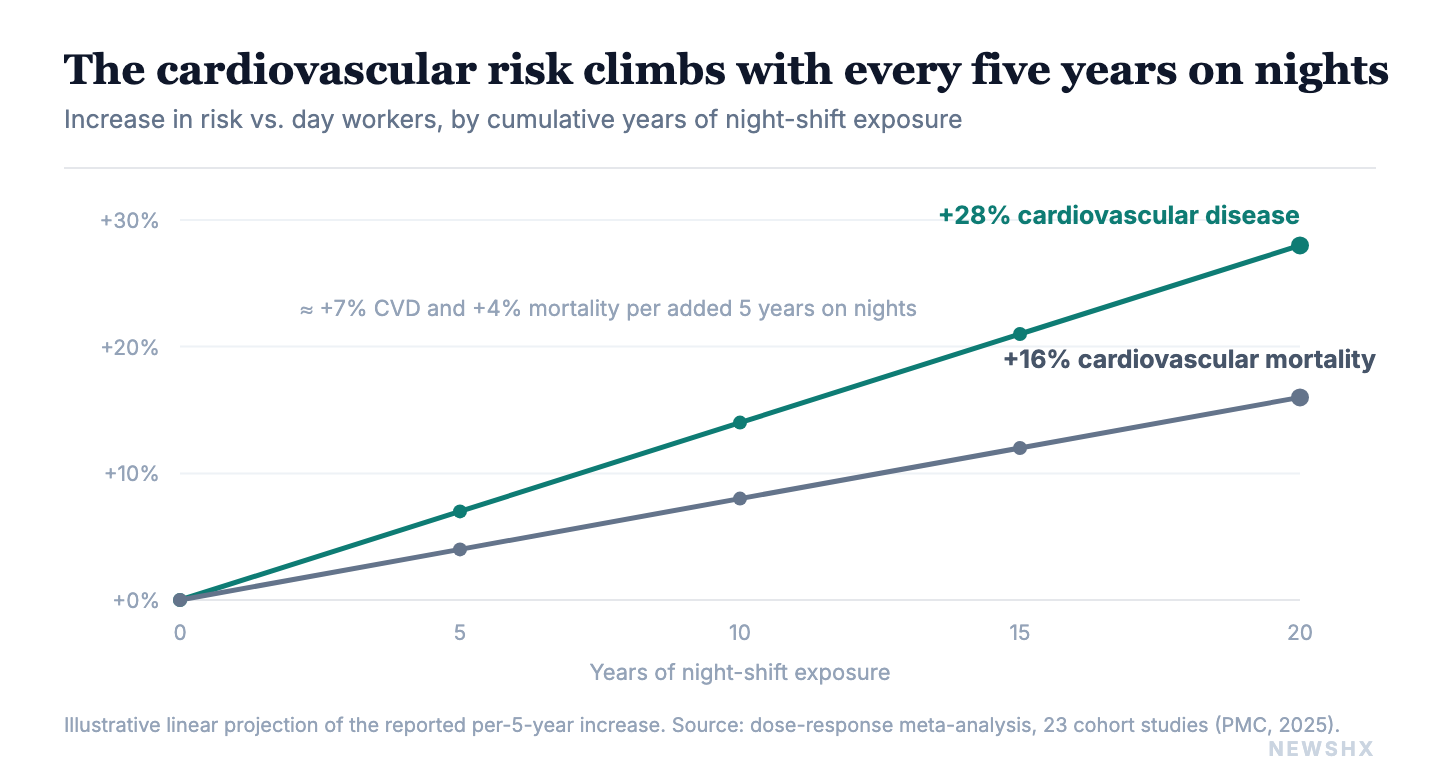
The cardiovascular evidence is the clearest. A 2025 dose-response meta-analysis of 23 cohort studies found that night shift work significantly raised the risk of both total cardiovascular events and cardiovascular mortality, and that the risk climbed with exposure: each additional five years of shift work was associated with roughly a 7 percent higher risk of cardiovascular disease and a 4 percent higher risk of dying from it.2 An umbrella review of systematic reviews reached the same direction across multiple outcomes, linking shift work to coronary disease, diabetes, and metabolic dysfunction.3
Then there is the finding that should reframe the entire conversation about differentials. A 2025 prospective cohort study of 192,764 adults measured biological age directly, using blood-based aging markers rather than self-report, and tracked participants for nearly 13 years.4 Permanent night shift workers were biologically older than their day-working peers, and the effect was dose-dependent. Translated into the number leaders should sit with: permanent night shift workers had an estimated loss of about 0.94 years of life expectancy at age 45.4 Close to a full year, gone, for the people working the hardest hours.
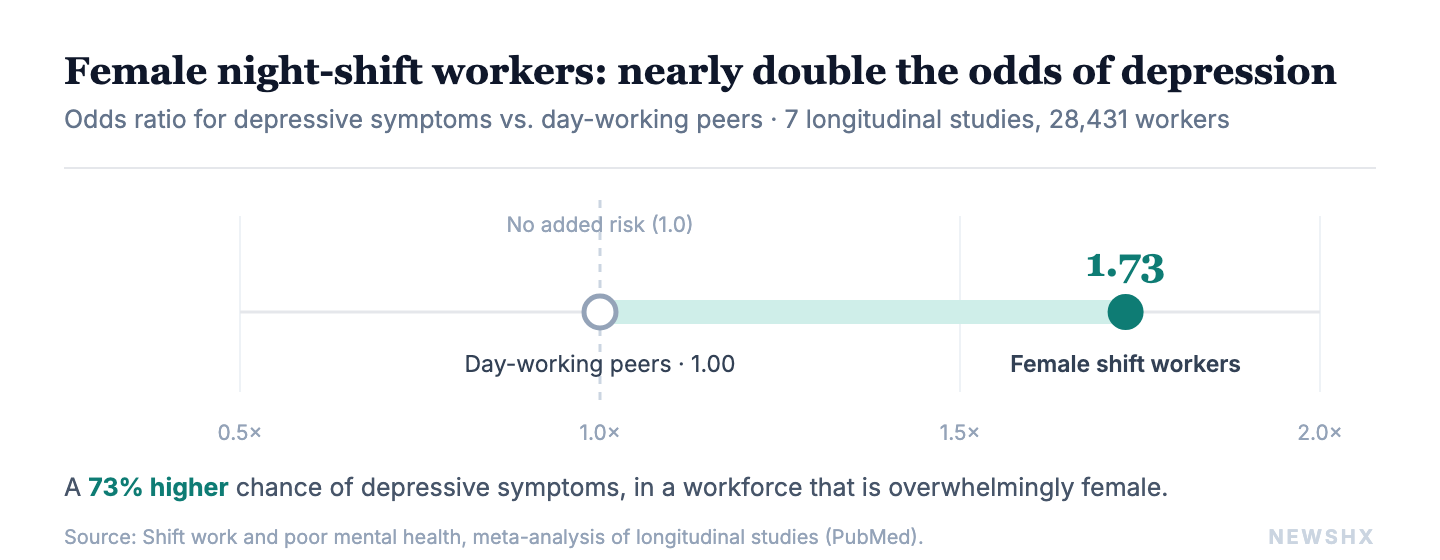
The toll, in three numbers: about 0.94 years of life expectancy lost at age 45 for permanent night workers, from a 192,764-person cohort; a 1.73 times higher odds of depression in female shift workers versus non-shift peers; and roughly 1 in 3 critical-care night staff screening positive for moderate-to-severe depression.
The night shift does not just borrow energy you pay back with sleep. On a population scale, it withdraws roughly a year of life. No differential I have seen is priced as if that were true.
The same study offered the one piece of genuinely hopeful news in this literature. A large share of the aging effect, roughly a third to a half, was mediated through body weight.4 That means a meaningful portion of the damage runs through pathways, metabolic and behavioral, that a well-designed workplace can actually influence. The biology is not entirely destiny. But that only matters if employers act on it, and most do not.
The part we undercount the most: mental health
Cardiovascular risk gets the headlines because it is easy to measure and easy to bill. The larger and more immediate toll is psychological, and it is the part the differential ignores completely.
The longitudinal evidence is direct. A meta-analysis of seven longitudinal studies covering 28,431 workers found that shift work was associated with a significantly higher risk of poor mental health, with the strongest signal for depressive symptoms.5 The effect was not trivial and it was not evenly distributed: female shift workers were markedly more likely to develop depressive symptoms than their non-shift-working peers, with an odds ratio of 1.73, meaning close to double the odds.5 In a workforce like nursing that is overwhelmingly female, that is not a footnote. That is the center of the problem.
A 2023 systematic review focused specifically on nurses pulled together 20 studies and confirmed the association between night shift work and depression in the population we ask to staff the most nights.6 And when you look at how the people on the floor are actually doing, the prevalence numbers are sobering. In a survey of night-shift healthcare workers in Paris, weighted prevalence reached 18.9 percent for depression, 11.7 percent for symptoms of post-traumatic stress, and 8.6 percent for severe insomnia.7 Among critical care providers specifically, one study found 42 percent reporting moderate-to-severe insomnia, 48 percent reporting fatigue, and 32 percent reporting moderate-to-severe depression.8
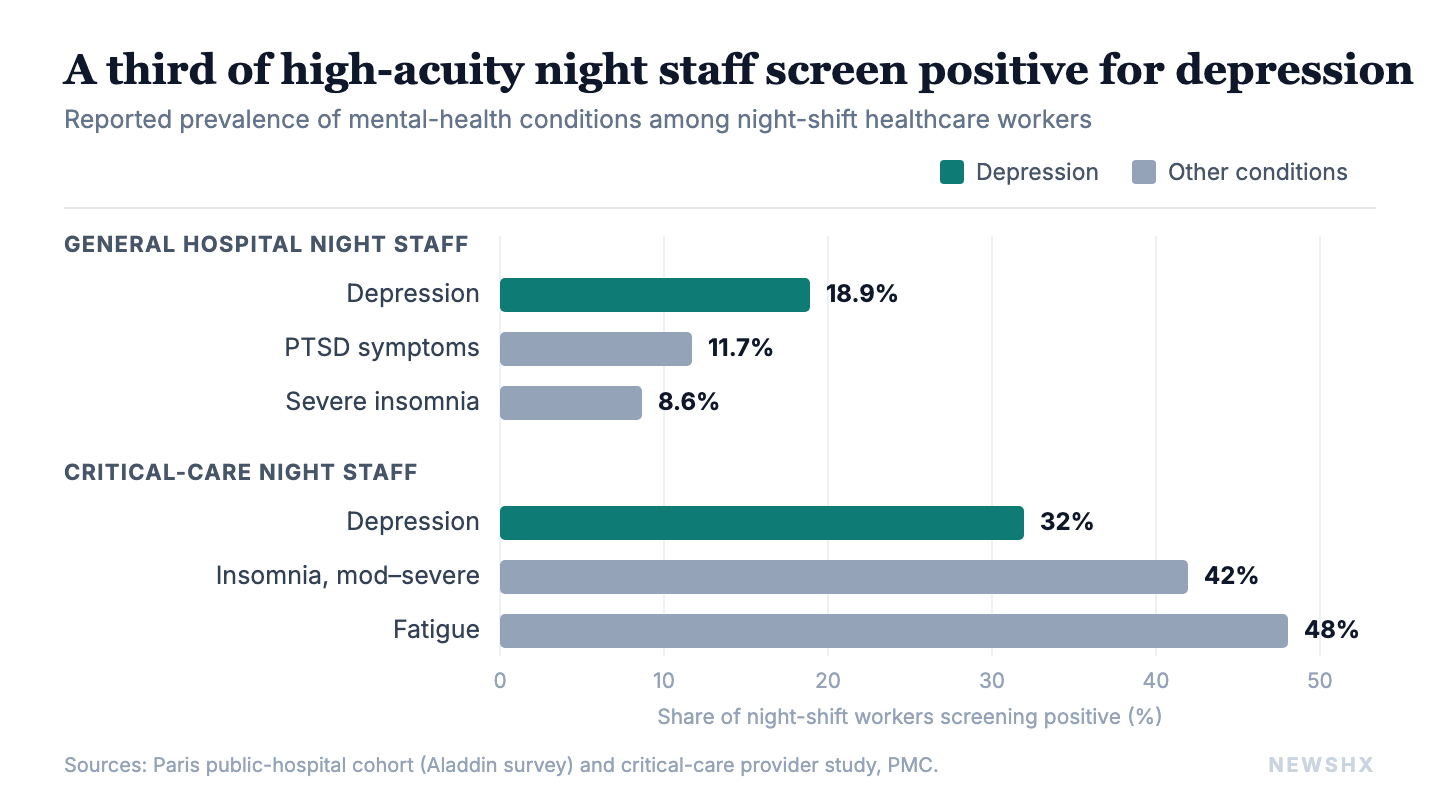
Put those two threads together. The night shift roughly doubles depression odds in the group most likely to work it, and a third of the people in the highest-acuity settings are already there. This is not a wellness-newsletter problem. It is a patient-safety problem, a retention problem, and a moral one.
So is $2 to $5 an hour justified?
Asked plainly: no, not as a substitute for managing the risk. As a wage premium, a differential is fine. As a settlement for the biological and psychological toll documented above, it is a category error. You cannot buy back a year of life expectancy or a doubled depression risk at four dollars an hour, and pretending the differential does that lets organizations skip the work that would actually help.
What the differential pays: about $3.50 to $5.25 extra per hour for a $35-an-hour nurse, roughly $140 to $210 across a 40-hour night week. What it is being asked to cover: about 0.94 years of life expectancy lost under permanent night work, roughly double the depression odds in women, a 7 percent higher CVD incidence and 4 percent higher CVD mortality per five years on nights, and 1 in 3 critical-care night staff already depressed.
The honest position is that the differential should stay, and it should be the smallest part of how an employer answers for night work. The differential is a price. What the evidence calls for is a program.
What employers can actually do
The same research that documents the harm points at the levers. None of this is exotic. Most of it is operational discipline that hospitals already know how to apply elsewhere.
The five levers, in brief: schedule for biology (cap night blocks near three consecutive nights, 8 to 9 hour shifts, at least 11 hours between shifts, with recovery days after); treat metabolic health as an occupational exposure; build behavioral health sized to the real prevalence; cap lifetime night exposure; and measure it, quantitatively and qualitatively.
Schedule for biology, not just for coverage. There are real numbers here, not just principles. The American Academy of Sleep Medicine recommends capping night work at blocks of about three consecutive nights, keeping individual shifts to roughly eight to nine hours, leaving at least eleven hours between shifts, and building in dedicated recovery days after a night block.12 The evidence behind those numbers is specific: injury risk climbs with each added consecutive night and peaks on the fourth, because alertness erodes shift over shift.12 In practice this means a schedule built around shorter blocks with protected recovery, something closer to a few nights on followed by real days off, is measurably safer than the seven-straight-nights-then-a-week-off pattern many units still run, where the worker is most impaired on the very last and longest stretch. Forward-rotating schedules (day to evening to night) are also easier on the clock than backward rotation.
Treat weight and metabolic health as an occupational exposure, not a personal failing. Since roughly a third to a half of the aging effect runs through body weight,4 night-shift-specific support, real food at 3 a.m. instead of vending machines, protected break spaces, sanctioned nap policies, on-shift movement, is not indulgence. It is risk mitigation with a measurable mechanism.
Build mental health support sized to the real prevalence. If a third of your critical-care night staff screens positive for depression,8 an annual EAP flyer is not a response. Confidential, low-friction, night-accessible behavioral health, screening that actually reaches the overnight workforce, and managers trained to see the early signs are the floor. And to be direct about what this is not: the answer is not to start every struggling night-shift clinician on an SSRI or SNRI and call it managed. Reaching for Effexor or its cousins to medicate people into tolerating a schedule that is making them sick is treating the symptom while protecting the cause. Some clinicians will genuinely need and benefit from medication, and that care should be available without stigma. But when the depression is being generated by the working conditions, the first-line intervention is the schedule, the recovery, and the support, not a prescription that lets a broken rotation continue unchanged.
Cap lifetime night exposure where you can. The dose-response shape of the cardiovascular and aging data2,4 means tenure matters. Rotating long-tenured staff off permanent nights, or capping years on the schedule, is a defensible workforce-health policy, not a scheduling inconvenience.
Measure it, quantitatively and qualitatively. Track night-shift-specific turnover, sick time, and incident rates against day shift. Go further and screen the overnight workforce directly with validated depression and burnout instruments, the PHQ-9 and similar, run at intervals rather than once, so you can see the trend, not just a snapshot. But the numbers alone will miss the picture. Pair them with structured employee interviews and listening sessions, because a depression score tells you that something is wrong and a conversation tells you what and why. The combination of quantitative screening and qualitative interviews is what gives leadership the complete picture. What gets measured gets budgeted, and right now most systems cannot tell you the marginal cost of a night-shift vacancy, which is exactly why they underinvest in preventing it.
Where AI and remote work change the math, and where they cannot
Here is the most important operational shift available, and the one most relevant to a technology-forward health system. A meaningful share of overnight clinical cognitive work no longer has to be done from inside the building, by a person who had to derange their own circadian rhythm to be there.
The models already exist and the outcome data is encouraging. Tele-ICU programs let intensivists monitor and co-manage critically ill patients remotely, and implementation has been associated with lower mortality, particularly in higher-risk patients, while reducing some of the EMR burden on on-site staff.9 Telestroke and teleneurology give a community hospital 24/7 access to board-certified stroke neurologists with rapid imaging review and acute decision support, coverage many of those hospitals could never staff on site.10 Tele-nocturnist and tele-hospitalist services put a physician on call for overnight admissions and questions with response times under a few minutes, instead of paying for an exhausted body in an empty hospital or an expensive locum.11 Teleradiology has run on this model for two decades.
The strategic point for workforce health is this: every overnight role that can be done remotely is a role where the clinician can live on a more humane schedule, or where a smaller, better-rested, deliberately managed overnight team can cover far more sites. AI extends the same logic, triaging which overnight events need a human now versus at 7 a.m., flagging deterioration earlier so fewer 3 a.m. crises require a full on-site response, and absorbing the documentation load that compounds night fatigue.
But the honest boundary has to be drawn, because over-promising here is its own failure. The hands-on, life-saving work of acute care cannot leave the building. The emergency physician running a code, the nurse titrating a drip, the surgeon called in for a ruptured aneurysm, the team physically managing an acute stroke or a crashing trauma, these cannot be done from a laptop and should never be marketed as if they can. The goal is not to empty the hospital at night. It is to make sure the only people who have to be there at 3 a.m. are the ones who genuinely have to be, supported by remote expertise and AI doing the cognitive and monitoring work that no longer requires a sacrificed circadian rhythm.
That distinction, what must stay physical versus what can move remote, is one of the highest-leverage workforce-design decisions a health system will make this decade. Get it right and you shrink the population exposed to the toll this article describes, without shrinking the safety net. Get it wrong and you either burn out your people or compromise the patients. And we should be honest that right now, we are getting it wrong. We are burning out the clinicians we need the most. Nurses are leaving bedside nursing. Physicians are walking away from the ED and the ICU for non-clinical work. The job is already heavy enough on its own terms, life-and-death decisions where getting it wrong can mean a death, and we are stacking avoidable burden on top of that for supportive roles that do not even have to be done on site, when better options exist.
What 14 nights taught me that the data could not
I do not write this from the outside. Before writing this article, I worked 14 straight nights, 9 p.m. to 7 a.m. I do it every year, on purpose, to remind myself of the work we ask people to do and the support a system has to provide at every level, work that comes at the real expense of the body of the person doing it.
The data in this piece names cardiovascular risk and lost life-years, and those are real. But the largest effect I felt was not in a lab value. It was the mental toll. The emotional lability, the bodily aches, the sense of being slightly out of phase with the entire world. And here is the part leaders need to understand. Somewhere in those two weeks, I stopped thinking about the money. The differential, the importance of having a job, none of it was in my head. That is exactly the state that drives burnout, and it is exactly the state that drives good clinicians out of practice and into a search for a better working environment.
The thing that changes that equation is not a bigger differential. It is someone checking in. It is an employer providing extra support, visibly, so that the people working the hardest hours know they are seen and cared for. That is the difference between a night-shift workforce you keep and one you lose.
The program I would build
I think in systems, not gestures, so my answer to all of this is not a flyer or a one-off wellness day. It is a standing program, owned and budgeted, with a name and an owner, designed specifically for the overnight workforce instead of inherited from the day-shift playbook.
The spine of it is a dedicated behavioral health clinician, a psychologist assigned to night staff rather than the generic, hard-to-reach EAP line. Every night-shift employee gets a proactive, scheduled check-in each quarter. Proactive is the key word: the session is on the calendar by default and the employee opts out, rather than having to raise their hand while already struggling, because the people who most need help are the least likely to ask for it. On top of the quarterly baseline, an as-needed pool sits open, on the order of 20 confidential sessions per quarter or per six months, available on demand at no cost, and bookable around night hours, including by telehealth at 3 a.m. when that is when the person is actually awake and hurting.
The program, in three parts: a dedicated night-shift psychologist with proactive, opt-out quarterly check-ins plus an on-demand pool of about 20 confidential sessions bookable at 3 a.m.; an integrated and layered design where each touchpoint runs the validated screen and trained managers and peer support mean the psychologist is not the only door; and funding set against turnover, since replacing one experienced ICU or ED clinician dwarfs a year of the program for an entire night cohort.
Three things make it real rather than decorative. First, it is integrated with the measurement layer above: each quarterly touchpoint runs the validated screen, so the program generates the trend data that justifies its own budget and surfaces a unit in trouble before it loses people. Second, it is layered, clinician for the clinical need, trained managers and a peer-support tier for the early signs and the day-to-day, so the psychologist is not the only door. Third, it is funded against the real number it offsets: the fully loaded cost of replacing a single experienced ICU or ED clinician dwarfs a year of this program for an entire night-shift cohort, which is what turns it from a cost center into the cheapest retention play on the table.
That is the altitude this problem has to be solved at. Not whether to add a dollar to the differential, but whether to stand up the system that keeps the people the differential was never going to keep on its own.
The bottom line
The night shift is not going away, and it should not. But we have been pricing it as if a few dollars an hour squared the account, and the evidence says it does not. Overnight work accelerates aging, shortens life expectancy by roughly a year for permanent night staff, and roughly doubles depression risk in the workforce most likely to do it. The differential is a wage. The toll requires a strategy: schedules designed for human biology, mental health support sized to the real numbers, metabolic risk treated as an occupational exposure, and an aggressive move to shift every overnight role that can be done remotely off the floor and onto a screen, so that the people who must be physically present are fewer, better rested, and better supported.
The organizations that figure this out will not just be more humane. They will keep their people. In a workforce this strained, that is the whole game.
Is your night-shift workforce getting a program, or just a premium?
A3HCS helps hospitals and health systems quantify what overnight work actually costs them, in turnover, in safety, and in lost clinicians, and design the workforce-health strategy that keeps the people they cannot afford to lose. The differential was never going to keep them. A system might.
Start the conversation at A3HCS.orgReferences
- Shift differential meaning in nursing: FAQ. IntelyCare. Accessed June 16, 2026. https://www.intelycare.com/facilities/resources/shift-differential-meaning-in-nursing-faq/. Night shift differential pay. NurseSalaryIntel. Accessed June 16, 2026. https://nursesalaryintel.com/salary-negotiation/night-shift-differential-pay
- Association between night shift work and cardiovascular disease: a systematic review and dose-response meta-analysis. Published 2025. Accessed June 16, 2026. https://pmc.ncbi.nlm.nih.gov/articles/PMC12506678/
- Shift work and health outcomes: an umbrella review of systematic reviews and meta-analyses of epidemiological studies. Accessed June 16, 2026. https://pmc.ncbi.nlm.nih.gov/articles/PMC8804985/
- Night shift work, accelerated biological aging and reduced life expectancy: a prospective cohort study. QJM. 2025;118(8):575. Accessed June 16, 2026. https://academic.oup.com/qjmed/article-abstract/118/8/575/8107780
- Shift work and poor mental health: a meta-analysis of longitudinal studies. PubMed. PMID 31536404. Accessed June 16, 2026. https://pubmed.ncbi.nlm.nih.gov/31536404/
- The relationship between working night shifts and depression among nurses: a systematic review and meta-analysis. Healthcare (Basel). 2023. Accessed June 16, 2026. https://www.ncbi.nlm.nih.gov/pmc/articles/PMC10094007/
- Negative representations of night-shift work and mental health of public hospital healthcare workers in the COVID-19 era (Aladdin survey). Accessed June 16, 2026. https://www.ncbi.nlm.nih.gov/pmc/articles/PMC9946706/
- The impact of night work on the sleep and health of medical staff. Accessed June 16, 2026. https://pmc.ncbi.nlm.nih.gov/articles/PMC11313391/
- An evaluation of the impact of the implementation of the Tele-ICU: a retrospective observational study. Accessed June 16, 2026. https://www.ncbi.nlm.nih.gov/pmc/articles/PMC9989570/
- TeleNeurology and telestroke coverage. Access TeleCare. Accessed June 16, 2026. https://accesstelecare.com/specialties/teleneurology/
- Four benefits of tele-critical care and tele-hospitalist night coverage. HUCU.ai. Accessed June 16, 2026. https://www.hucu.ai/four-benefits-of-tele-critical-care-and-tele-hospitalist-night-coverage/
- Shift work provider fact sheet. American Academy of Sleep Medicine. Accessed June 16, 2026. https://aasm.org/wp-content/uploads/2022/07/ProviderFS-ShiftWork.pdf. Supporting evidence on consecutive night shifts and injury/fatigue risk. Accessed June 16, 2026. https://www.ncbi.nlm.nih.gov/pmc/articles/PMC8527589/