
A hospitalist I worked with once showed me a small scheduling tool she had built to stop patients from falling through the cracks after discharge. It worked. It measurably cut her unit's bounce-backs. Then I asked the obvious question, the one my MBA had trained into me: who owns it, and did anyone protect it? She looked at me like I had asked whether she owned the weather. It never occurred to anyone that she had invented something. That reflex, the assumption that discovery is someone else's business, is the most expensive blind spot in healthcare. Because the truth is that the cures we prescribe were almost all invented by people exactly like her, and a quiet machine most clinicians cannot name is what decides whether those inventions ever reach a patient.
That machine is called technology transfer. It is the process that turns a basic-science discovery into a patent, a patent into a license, and a license into the drug, device, or diagnostic you will order this week. When it works, nobody sees it. When it stalls, the pipeline of new therapies quietly thins, and by the time that shows up in your formulary it is a decade too late to fix. I want to make the case that healthcare leaders should understand this system as infrastructure, not trivia. It is the supply chain of medical innovation, and right now it is under strain.
Public science invents. Technology transfer translates. Industry scales. Miss the middle term and you misunderstand where your therapies actually come from.
Who really invents your drugs
Start with a number that should end the debate. A study in the Proceedings of the National Academy of Sciences examined every one of the 210 new drugs the FDA approved between 2010 and 2016. Every single one had benefited from federally funded research, and that public science was concentrated in the most innovative products, the first-in-class mechanisms rather than the follow-ons. The National Institutes of Health did not market these drugs. But the foundational biology, the target, the mechanism, the early validation, came out of academic and government labs before any company took the commercial risk.
This is not an accident of history. It is the design of a single 1980 law. The Bayh-Dole Act let universities own and license the inventions that came out of their federally funded research, instead of leaving that intellectual property to sit unused in a government drawer. That one change built an economy. By the accounting the field cites most often, university-based federally funded research has since helped launch tens of thousands of startups, support millions of jobs, and add hundreds of billions of dollars to the economy. More to the point for anyone who runs a clinical service: it is why the pipeline exists at all.
Follow one product from grant to bedside
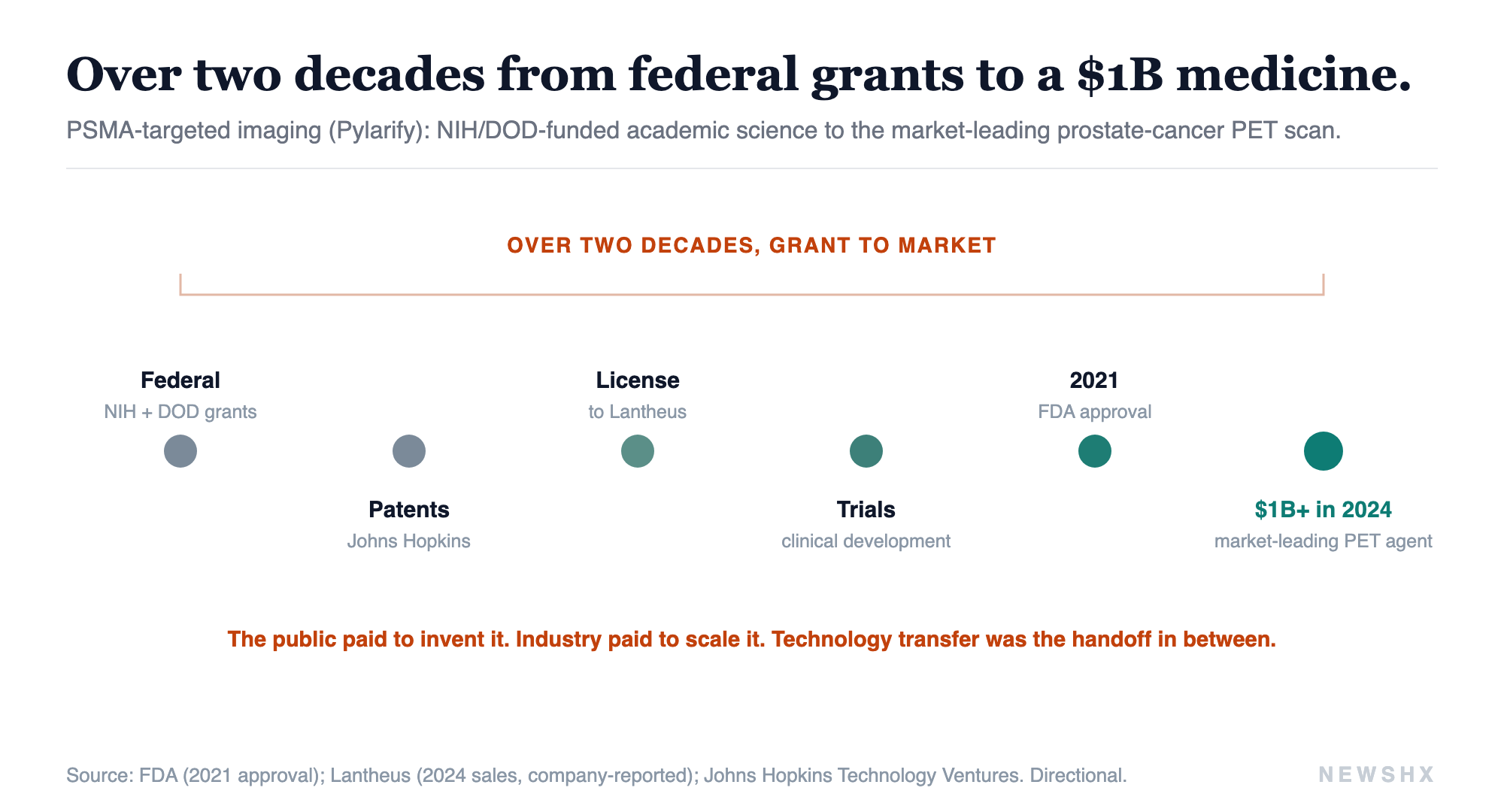
The clearest way to see the machine is to trace a single product. Consider targeted drug delivery, the frontier rewriting oncology: get the therapy to the diseased cell, spare everything else. The version now in wide use for prostate cancer, PSMA-targeted imaging and radioligand therapy, did not spring from a corporate lab. It was built over more than two decades on a series of NIH and Department of Defense grants to academic researchers, then patented, then licensed to industry, which carried it through trials and manufacturing to market. It is now the leading diagnostic of its kind, used in hundreds of thousands of patient scans a year. The public paid to invent it. The company paid to scale it. Technology transfer was the handoff in between, and without that handoff the science stays a paper.
The pattern repeats across the therapies that define modern care. The entire class of checkpoint-inhibitor immunotherapy traces to basic immunology done in academic labs, work that earned a Nobel Prize before it earned a dollar. One of the most consequential metabolic drug classes of our era, the GLP-1 receptor agonists now reshaping diabetes and obesity care, grew from a discovery an academic scientist made studying the venom of a desert lizard, on government time, decades before a blockbuster existed. The recent wave of targeted therapies for previously untreatable brain tumors runs on genetics that federal grants funded for years before a pill existed. In each case the commercial partner is real and necessary. In each case the origin is a campus.
Now the honest skeptic, because credibility depends on it
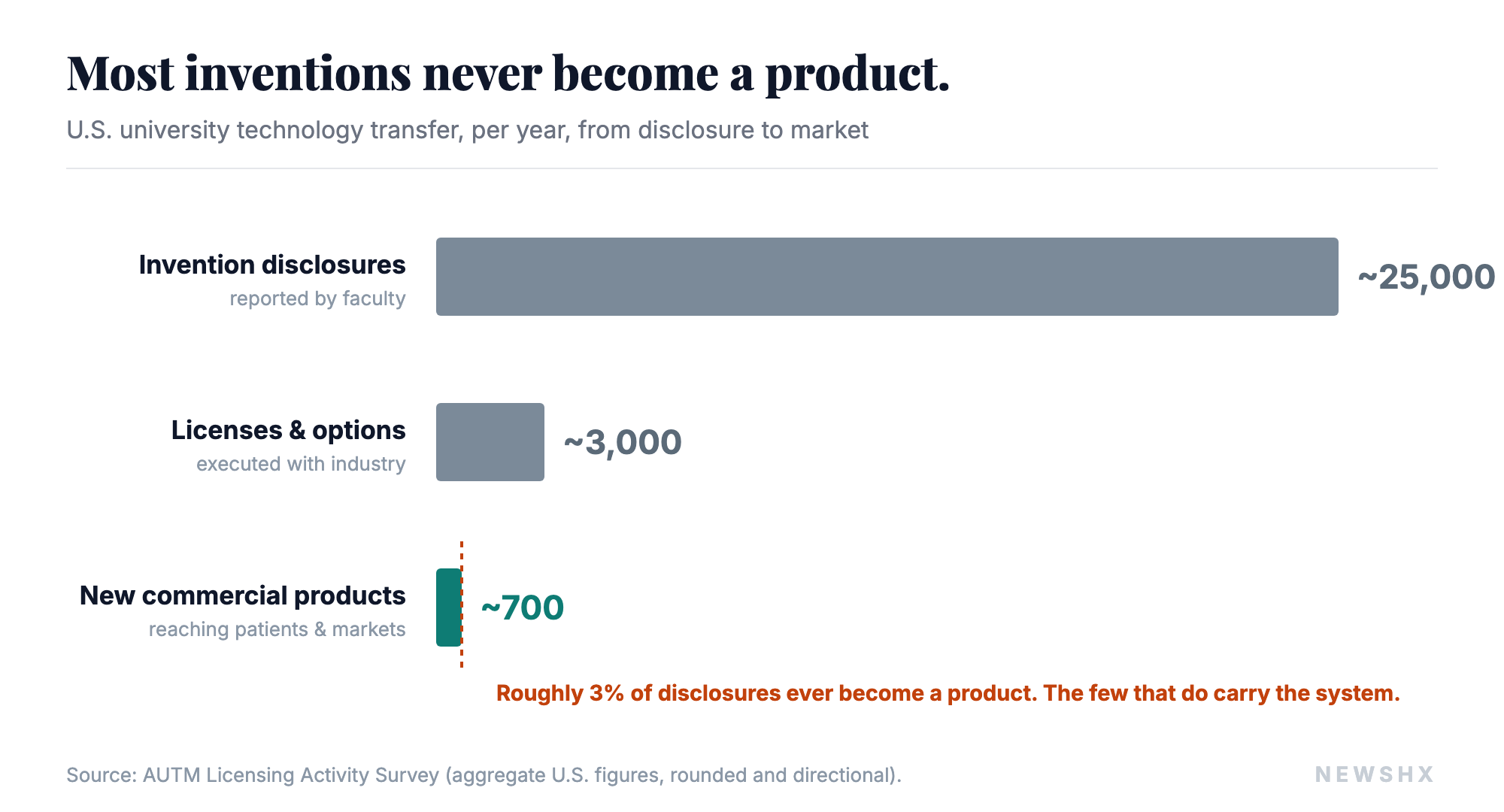
Technology transfer is not a clean machine, and pretending it is would be its own kind of malpractice. Most academic inventions never get licensed at all. In a typical year the nation's universities file more than twenty thousand invention disclosures and execute only a few thousand licenses, and only a fraction of those ever become a product a patient uses. The revenue is brutally concentrated: a small number of blockbuster licenses at a handful of institutions carry the entire system, while most technology-transfer offices barely break even. Between discovery and market sits the "valley of death," the stretch where promising science runs out of funding before it is de-risked enough for a company to take on. And academic science has a reproducibility problem that means some of what gets patented does not hold up.
So I am not claiming the system is efficient or fair. I am claiming it is essential, and that its inefficiency is exactly why it must be strengthened rather than taken for granted. The handful of cures that make it through pay for all the shots on goal that miss. Starve the inputs and you do not trim the waste, you lose the winners.
Why this is an operator's problem, not an academic one
The federal research funding that seeds this entire pipeline is facing real uncertainty, and universities are responding by leaning harder on industry partnerships to fill the gap. That is not an abstract policy story. The therapies your organization will be buying, deploying, and building service lines around in 2032 are being invented, or not invented, in that funding environment right now. The innovation you will prescribe a decade from now is a function of the grants written and the partnerships struck today.
And here is the part most operators miss: your own institution is probably an inventor, too. Academic medical centers and even community health systems generate intellectual property constantly, in care-delivery models, digital tools, devices clinicians jury-rig at the bedside, and workflow innovations nobody names as inventions. Most of it evaporates because no one is watching for it, like the hospitalist and her scheduling tool. The same discipline that moves a university discovery to market, spotting the invention, protecting it, finding the partner, structuring the deal, is a capability health systems can build and mostly have not.
The drug that saves your patient did not begin in a boardroom. It began as a grant application, in a lab, on a campus.
Where I land
The story we tell about medical breakthroughs is a story about companies. The truer story is a partnership: public science invents, technology transfer translates, industry scales. Miss the middle term and you misunderstand where your therapies come from, and you underinvest in the one part of the chain that is quietly deciding what medicine will exist to practice.
If you lead in healthcare, the move is to treat innovation as a supply chain you have a stake in, not a miracle that arrives fully formed. Understand where your pipeline originates. Watch for the intellectual property your own clinicians are generating and letting slip. And take seriously that the unglamorous machinery of commercialization, the licenses and term sheets and partnerships nobody celebrates, is where the next decade of cures is being decided. The question for all of us is whether we protect the machine that carried the cure from there to here.
Your clinicians are inventing. Is anyone protecting it?
A3HCS helps hospitals and health systems treat innovation as infrastructure: spotting the intellectual property your teams generate, shaping industry and academic partnerships, and building the commercialization discipline that turns a bedside workaround into a protected, partnered asset instead of a lost one. If your organization is inventing and letting it slip, that is a fixable problem.
Start the conversation at A3HCS.orgReferences
- Cleary EG, Beierlein JM, Khanuja NS, McNamee LM, Ledley FD. Contribution of NIH Funding to New Drug Approvals 2010-2016. Proc Natl Acad Sci USA. 2018;115(10):2329-2334. doi:10.1073/pnas.1715368115
- Bayh-Dole Act, Patent and Trademark Law Amendments Act of 1980. Public Law 96-517; codified at 35 U.S.C. 200-212.
- Association of University Technology Managers (AUTM) / BIO. The Economic Contribution of University/Nonprofit Inventions in the United States. Figures are advocacy-report estimates; directional. autm.net
- Johns Hopkins Technology Ventures. FY2025 Annual Report. PSMA-targeted imaging and radioligand therapy (Pylarify) development and licensing to Lantheus Holdings. Sales and scan-volume figures are company/report-reported; confirm against Lantheus public filings. ventures.jhu.edu
- The Nobel Prize in Physiology or Medicine 2018: James P. Allison and Tasuku Honjo, for their discovery of cancer therapy by inhibition of negative immune regulation. NobelPrize.org
- Eng J, Kleinman WA, Singh L, Singh G, Raufman JP. Isolation and characterization of exendin-4, an exendin-3 analogue, from Heloderma suspectum venom. J Biol Chem. 1992;267(11):7402-7405.
- Mellinghoff IK, van den Bent MJ, Blumenthal DT, et al. Vorasidenib in IDH1- or IDH2-Mutant Low-Grade Glioma (INDIGO). N Engl J Med. 2023;389(7):589-601. FDA approval August 2024.
- AUTM Licensing Activity Survey, FY2023 (U.S. edition). Aggregate invention-disclosure, license, and new-product figures. autm.net / STATT database.
- Begley CG, Ellis LM. Raise standards for preclinical cancer research. Nature. 2012;483(7391):531-533.
- Federal research-funding uncertainty and rising reliance on industry-sponsored research: framing consistent with institutional statements including Johns Hopkins Technology Ventures FY2025 Annual Report. Directional; not a specific budget figure.