
A patient with hypertension, high cholesterol, and early type 2 diabetes sits in a community clinic. Across from them is a physician and a registered dietitian, together, in a kitchen. They do not just get a printout that says eat less sodium. They cook. They leave with a plan, and the clinic leaves with something it has almost never had before in this arena: a paid claim.
For most of the last decade, that last part was the problem. Nobody seriously disputes that diet is a leading driver of chronic disease. The dispute was always about who pays for the intervention. Nutrition counseling has lived on grants, philanthropy, and the unbillable goodwill of dietitians squeezed into a schedule that does not reimburse their time. Food is medicine could be true and still be financially impossible, which in American health care means it does not scale.
That is what changed. Not the science. The economics.
The evidence that food is medicine was never the bottleneck. The bottleneck was that nobody could bill for it. A clinic just proved you can.
The proof: 30 months of paid claims
The data comes from a culinary medicine service line built at an academic medical center and reported in NEJM Catalyst in September 2025 1. The design matters as much as the numbers, so start there. This was not a dietitian working alone. It was an interprofessional model, a physician and a certified dietitian nutritionist working together, structured into three billable encounter types: electronic consults between clinicians, one-to-one clinic visits, and shared medical appointments where ten to sixteen patients meet with the physician, the dietitian, and volunteers in a community kitchen 1.
The point of that structure is that each arm generates a billable event. Culinary medicine has historically failed to scale not because it does not work but because it was built in ways payers do not recognize. This team built it in ways they do.
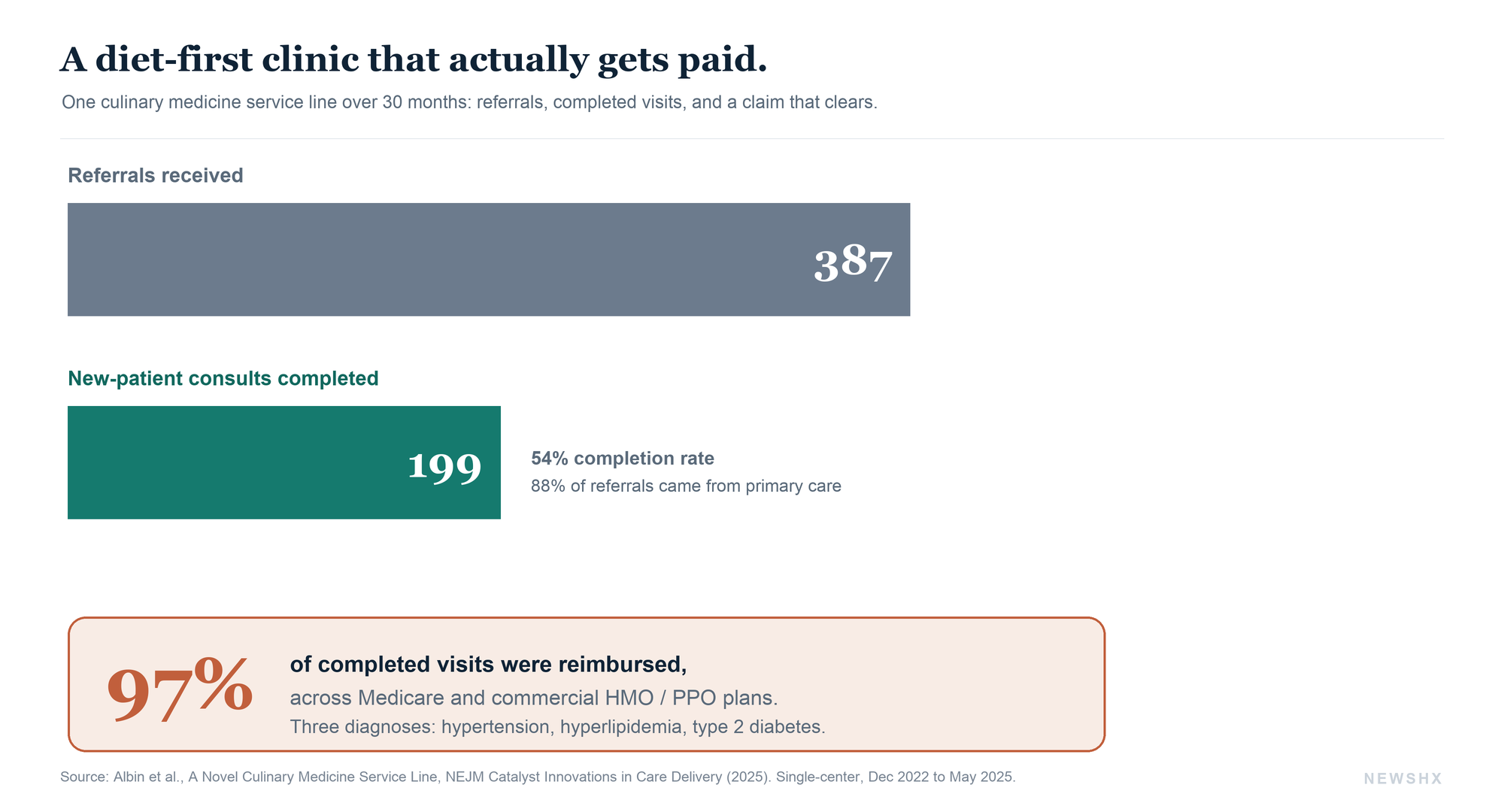
Over 30 months, from December 2022 to May 2025, the clinic took 387 referrals and completed 199 new-patient consults, a 54 percent completion rate. Primary care sent 88 percent of those referrals 1. The patients were, on average, 54 years old, mostly women, and majority African American, and the three most common referral diagnoses were the exact trio that defines American cardiometabolic disease: hypertension, hyperlipidemia, and type 2 diabetes 1.
Then the number that actually breaks the old pattern. 97 percent of visits were covered under Medicare and various commercial HMO and PPO plans 1. The gross collection rate as a share of the charge ranged from roughly 16 to 70 percent depending on payer mix, which is unglamorous but is exactly the kind of real-world revenue variability that tells you this is an operating service and not a demonstration. And 92 percent of surveyed patients were satisfied or very satisfied 1.
By the numbers. 387 referrals. 199 completed visits. 88 percent from primary care. 97 percent reimbursed across Medicare and commercial plans. Three diagnoses: hypertension, hyperlipidemia, type 2 diabetes. This is what food is medicine looks like once it has a claim number attached.1
Read that as an operator, not a clinician. A community-based, diet-first intervention for the most expensive chronic diseases in the country generated paid claims across nearly every major payer type for two and a half years. The reimbursement was not exotic. It ran through ordinary evaluation-and-management and shared-medical-appointment mechanics that any system with a dietitian and a willing physician could, in principle, replicate.
Why this is the hinge, not just a nice study
Zoom out to why the timing is not a coincidence. The past year produced three signals that food as medicine is crossing from advocacy into infrastructure.
First, the New England Journal of Medicine launched a dedicated Nutrition in Medicine review series in 2025 5,6. Its own framing editorial noted that suboptimal diet is tied to roughly 11 million deaths a year worldwide and drives close to one in five deaths, yet fewer than 1 percent of questions on medical licensing exams touch nutrition 5. When the most conservative journal in medicine decides nutrition needs its own standing review series, that is the field being promoted from soft science to core curriculum.
Second, the money and the policy are moving underneath it. Produce-prescription programs, medically tailored meals, and Medicaid Section 1115 waivers that pay for food have gone from fringe to fundable 3. The culinary medicine billing data is the clinic-level version of the same shift: the reimbursement scaffolding is finally being built.
Third, and this is the one clinicians should sit with, the cost case is overwhelming. The Mozaffarian-led JAMA Network Open study opens by noting that poor nutrition is a leading driver of morbidity and mortality, tied to an estimated 45 percent of cardiovascular disease mortality, 70 percent of new diabetes cases, and $1.1 trillion in annual US health care spending and lost productivity 2. When a single modifiable risk factor is implicated in numbers that large, the failure to reimburse the intervention stops looking like fiscal caution and starts looking like the more expensive choice.
Poor diet is tied to 45 percent of cardiovascular deaths, 70 percent of new diabetes cases, and $1.1 trillion a year. At that scale, not paying for nutrition is not the cautious option. It is the expensive one.
The catch: a claim number is not a grocery bag
Here is where the honest version of this story diverges from the triumphant one. Reimbursing a clinic visit and fixing a patient's nutrition are not the same act, and the second body of work from this same period exists to make sure nobody confuses them.
The reframe is from food insecurity to nutrition insecurity, and it is not semantic. Food insecurity asks whether you have enough calories. Nutrition insecurity asks whether you have consistent access to the healthy food that actually prevents disease, which is a larger and different problem. A recent NEJM review drew the line explicitly: nutrition insecurity affects a much larger share of the population than food insecurity, because it captures people who can technically buy food but cannot reliably get the right food 4.
Then the survey that put barriers to numbers. In a study of 3,000 US adults using a validated Nutrition Security Screener, the obstacles to healthy eating clustered into two factors that explained most of the variance, and they mapped hard onto disadvantage 2. Black adults had meaningfully higher odds of transportation barriers. Food insecurity was associated with sharply higher odds of barriers around physical function, the ability to cook, and the ability to get to a store, transportation carrying more than four times the odds 2. And crucially, a higher barrier count tracked with higher prevalence of diabetes, heart disease, obesity, and stroke 2.
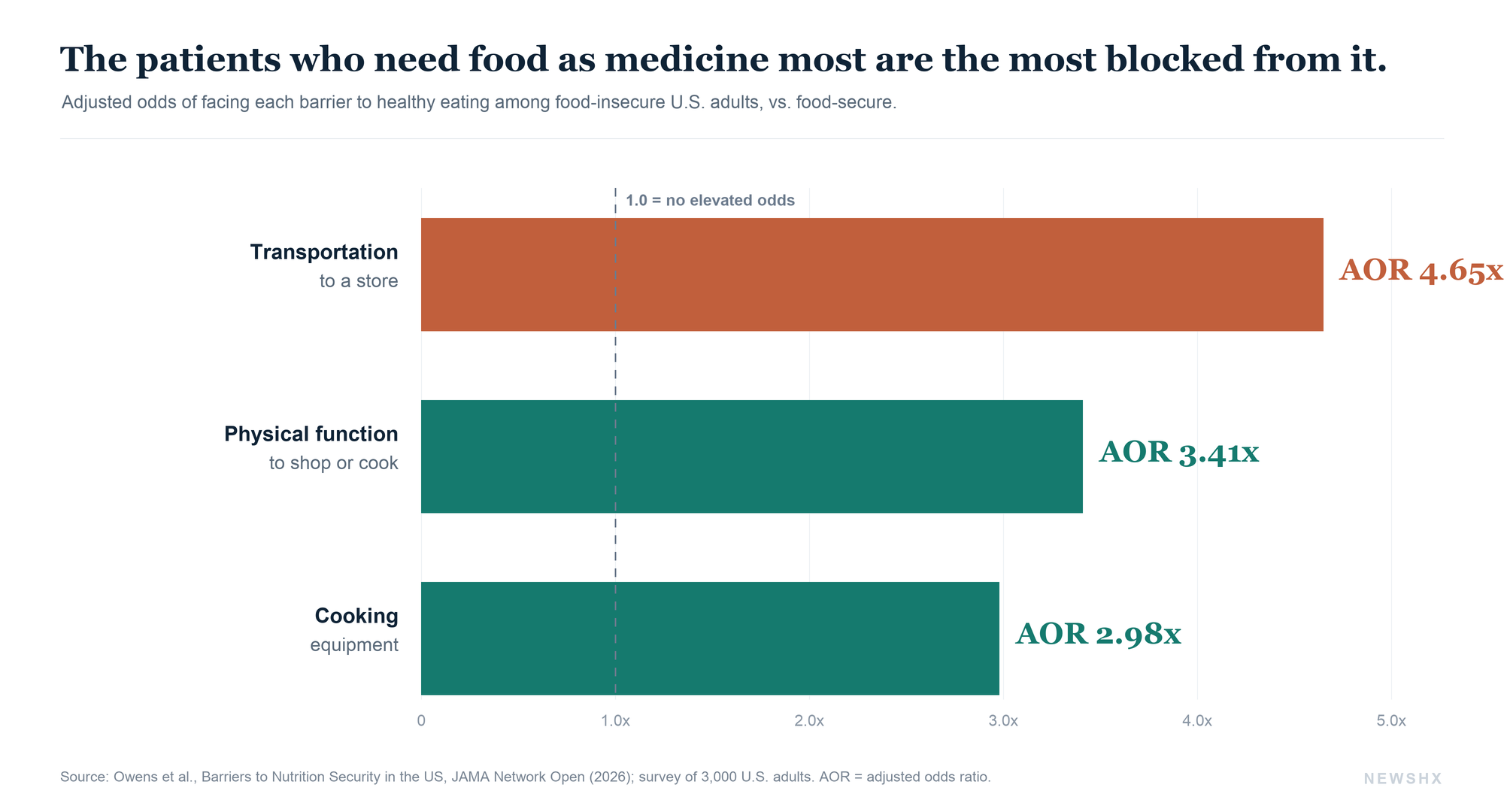
That is the finding a culinary medicine clinic cannot bill its way past. If a patient cannot get to the store, lacks a working kitchen, or cannot stand long enough to cook, a reimbursed cooking class is necessary and insufficient at the same time. The clinic visit teaches the skill. It does not remove the barrier. And the barriers concentrate in exactly the population the billing study served: majority African American, community clinic, cardiometabolic disease.
The patients most likely to benefit from food as medicine are the ones most likely to be blocked from it by transportation, a missing kitchen, and physical limitation. A billing code pays for the visit. It does not buy the groceries or drive the patient to them.
What this looks like from the bedside
I have spent most of my clinical career in the recovery lane, with patients moving from an acute event back to a home that is supposed to hold them. Nutrition is where a surprising number of those recoveries quietly come apart. A patient with a brain injury, a stroke, or a new diabetes diagnosis leaves with a diet that would genuinely change their trajectory, and then meets a life the discharge summary never accounted for: no ride to a store that stocks fresh food, a kitchen that is a microwave and a hot plate, an income that makes cheap dense calories the rational choice. The plan was correct. The conditions to act on it were missing, and the readmission that follows gets blamed on the disease rather than the gap.
That is the same failure the culinary medicine data and the nutrition-security data describe from two directions, which is why I read the reimbursement breakthrough as necessary but only half the build. Teaching a patient to cook, and finally getting paid to do it, is real progress. It does not put a working stove in the apartment or a grocery within reach. For the sickest, most marginal patients, the ones who fill these clinics, the intervention only lands if someone also closes the distance between the plan and the plate.
What actually has to be true for this to work
So hold both facts. The reimbursement barrier, the one everyone said was the real obstacle, is falling. And a second set of barriers, the structural ones, is now the binding constraint. A serious food-as-medicine strategy has to solve for both, which means it looks less like a wellness program and more like an operating model. Three things have to be true.
The interprofessional pairing has to be real, and the dietitian has to be an equal. The billing study worked because a physician and a registered dietitian shared the encounter and shared the revenue 1. Applied nutrition is the dietitian's discipline, not the physician's, and the models that treat the RD as a co-owner of the clinical relationship are the ones that produce both outcomes and paid claims. The systems that bolt nutrition onto a physician visit as an afterthought will get neither.
The billing has to be designed in, not discovered later. Culinary medicine did not become reimbursable by accident. This team architected it around recognized encounter types, including shared medical appointments that spread a physician's time across ten to sixteen patients and make the economics work 1. Any system trying to copy this needs to start with the claim, not end with it.
Someone has to own the barriers the clinic cannot bill for. This is where health systems, plans, and community organizations either close the loop or watch it stay open. Transportation, kitchen access, and the actual food itself sit outside the visit. The reimbursed clinic is the front door. Produce prescriptions, medically tailored meals, and the emerging Medicaid food benefits are what has to be waiting on the other side of it 3. Reimbursement for the encounter and provision of the food are two different line items, and a program that funds only the first will underperform and then get blamed for the science rather than the design.
Food is medicine was always true. What it lacked was a business model, and for the first time there is real evidence one exists. The clinics that win the next five years will be the ones that treat that evidence correctly: as proof that the door is now payable, and as a reminder that the door was never the hard part.
The door is now payable. The build is closing the loop behind it.
A culinary medicine clinic just proved food as medicine can run as a reimbursed service line, not a grant-funded pilot. But the reimbursed visit is only the front door. Transportation, kitchen access, and the food itself are separate line items, and a program that funds only the encounter will underperform and then get blamed for the science instead of the design. A3HCS helps health systems and plans architect nutrition service lines that bill from day one and own the barriers the claim cannot touch, with a physician-executive read on the interprofessional model, the encounter mechanics, and the value case.
Start the conversation at A3HCS.orgReferences
- Albin J, Wong W, Siler M, Bowen ME, Kitzman H. “A Novel Culinary Medicine Service Line: Practical Strategy for Food as Medicine.” NEJM Catalyst Innovations in Care Delivery. 2025;6(9). doi.org/10.1056/CAT.24.0347
- Owens CE, Ridberg R, Reedy Sharib J, Craig HC, Mozaffarian D. “Barriers to Nutrition Security in the US.” JAMA Network Open. 2026;9(6):e2620264. doi.org/10.1001/jamanetworkopen.2026.20264
- Byhoff E, Rudel RK. “Federal Policy and Social Support to Increase Nutrition Security.” JAMA Network Open (Invited Commentary). 2026;9(6):e2620269. doi.org/10.1001/jamanetworkopen.2026.20269
- Gallegos D. “Effects of Food and Nutrition Insecurity on Global Health.” New England Journal of Medicine. 2025;392(7):686–697. doi.org/10.1056/NEJMra2406458
- Lee CD, Hardin CC, Longo DL, Ingelfinger JR. “Nutrition in Medicine — A New Review Article Series.” New England Journal of Medicine (editorial). 2025. doi.org/10.1056/NEJMe2313282
- Heymsfield SB, Shapses SA. “Guidance on Energy and Macronutrients across the Life Span.” New England Journal of Medicine. 2025;392(9). doi.org/10.1056/NEJMra2214275