
Picture the most common serious house call in American medicine. A 62-year-old with crushing chest pain calls 911. An advanced life support crew arrives, starts a line, acquires a 12-lead ECG in the living room, and rolls for the nearest cath-capable hospital. Two system failures are now in motion, and neither has anything to do with the medicine. The first arrives in about ninety days, as a bill built on an average ALS base charge of $1,277 before mileage, for a service no one chose, negotiated, or could have refused 1. The second is already over: at most hospitals, almost nothing the crew just learned, the ECG, the vitals, the story, even the ambulance's location and arrival time, traveled ahead of the patient. The emergency department will find out what is coming when it comes through the door.
This article is about why both failures exist, and why they are, at bottom, the same failure. America prices ambulances like taxis, a base rate plus mileage, and a taxi meter funds neither the standing readiness that makes a 911 system work nor the data layer that makes the receiving hospital ready. The bill is too high and the information is too thin for the same structural reason.
We pay for the ride. We do not pay for the readiness, and we do not pay for the information. Then we act surprised that the bill is enormous and the ER is blind.
The meter, not the medicine
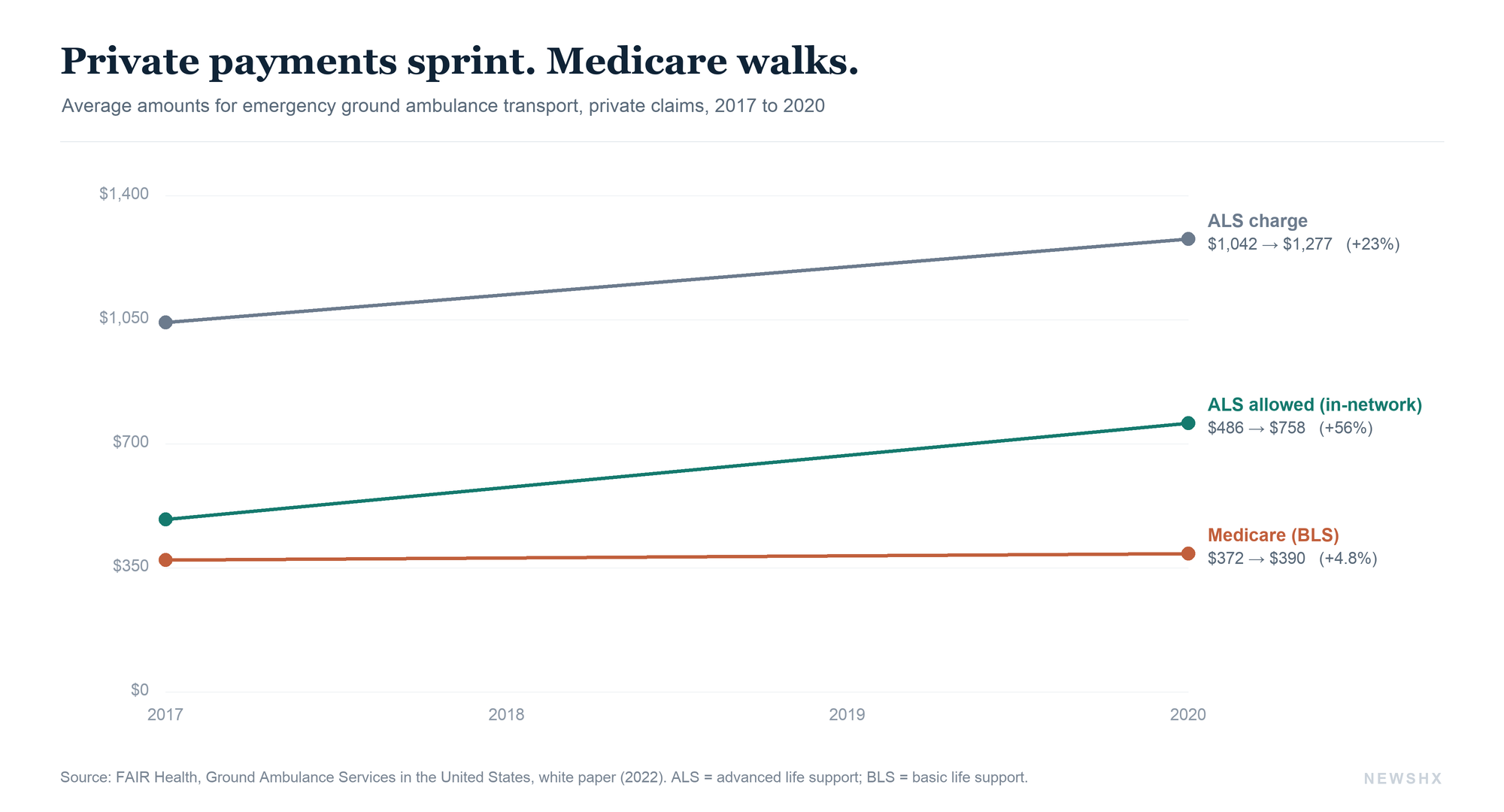
Start with what the meter reads. In FAIR Health's national study of private insurance claims, the average charge for an advanced life support emergency transport rose from $1,042 in 2017 to $1,277 in 2020, a 22.6 percent increase, while basic life support charges rose from $800 to $940 1. Those are base rates only. Mileage is billed on top, and in 2022 the average in-network mileage rate ranged from $5.79 per statute mile in Florida to $28.35 in Utah 2. What insurers actually allowed moved even faster than charges: the average in-network allowed amount for ALS transport climbed 56 percent in three years, from $486 to $758 1.
Now put Medicare beside those numbers. Over the same period, Medicare's payment for the equivalent BLS emergency service moved from $372 to $390, a 4.8 percent increase 1. That spread, private allowed amounts sprinting while Medicare walks, is not a detail. It is the business model, and the patient with commercial insurance is the one funding it.
Half the rides come with a second bill
The ambulance is the most out-of-network service in American healthcare. KFF found that 51 percent of emergency ground ambulance rides for privately insured patients involved an out-of-network charge, and ambulances carry about 3 million privately insured patients to emergency rooms every year 3. FAIR Health's more recent claims run put the out-of-network share at 59.4 percent of all ground ambulance claim lines in 2022, and 62 percent of emergency rides 2. A JAMA Network Open analysis of more than two million commercially insured transports found 54.8 percent billed out-of-network, with the patient's total financial burden averaging $434.70 per out-of-network ride versus $132.21 in-network 4.
The surprise bill that follows has a median around $450, but the distribution has a long tail: the median in California is $1,209, and insured patients collectively pay about $129 million a year in ambulance balance bills 5. And unlike almost every other surprise bill in medicine, this one attaches to a service nobody can shop for. No one comparison-prices an ambulance from the floor of their kitchen.
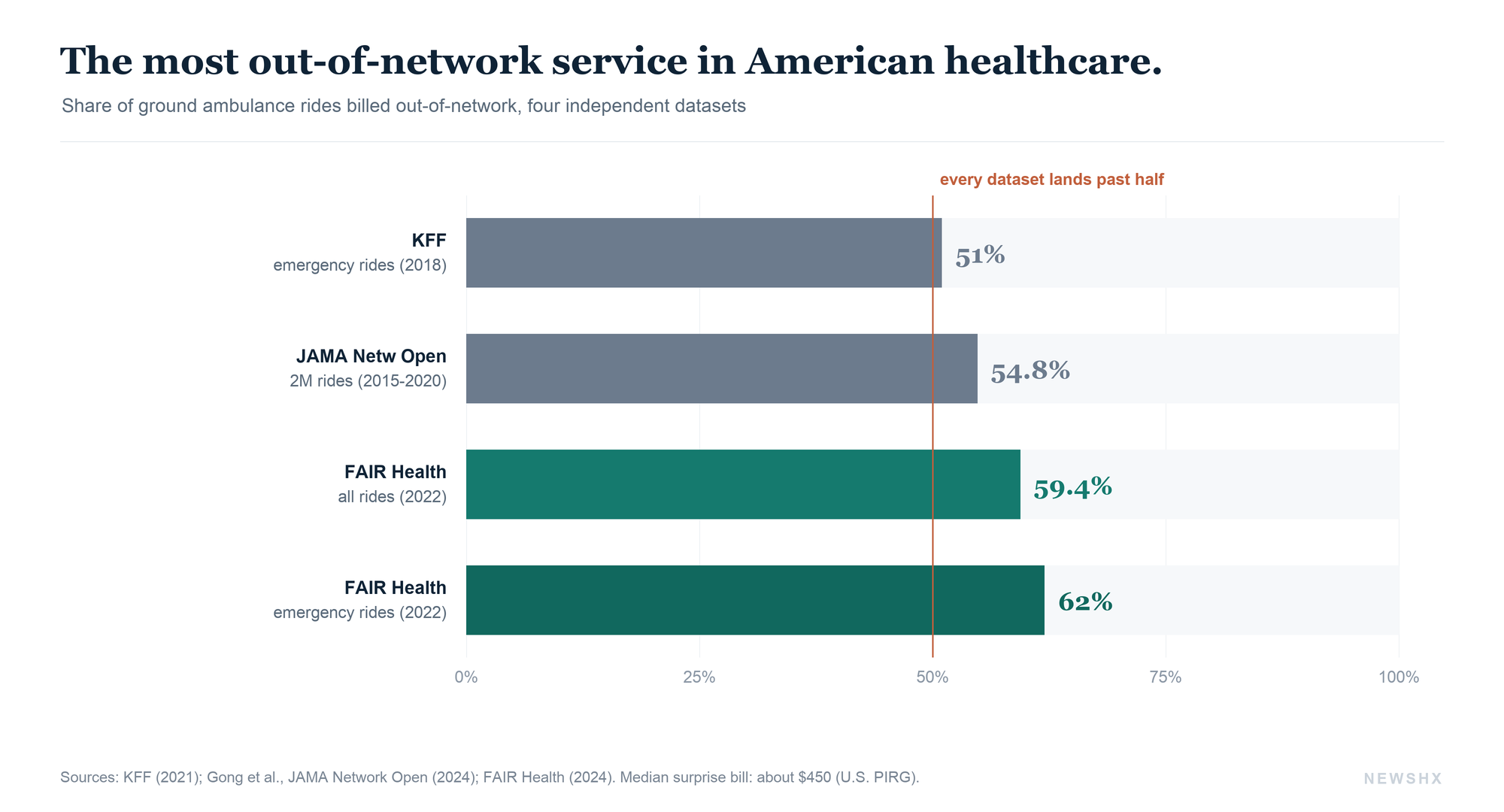
51 to 62 percent of emergency ground ambulance rides involve an out-of-network charge, depending on the dataset and year. Median surprise bill: about $450. In California: $1,209. Collective annual balance-bill burden on insured patients: roughly $129 million.
Why the price is set where it is
To understand the price, stop thinking of the ambulance as a vehicle and start thinking of it as a standing capability. EMS in the United States is a patchwork of more than 14,000 agencies reporting into the national EMS database, with no ownership analogue anywhere else in the system: 37 percent of emergency rides are run by fire departments, 25 percent by other government agencies, 30 percent by private companies, and 8 percent by hospitals 3,6. Some bill like public utilities, some like municipal services, some like private equity portfolio companies, because they are all of those things.
The dominant cost is not the ride. It is readiness, the expense of keeping a staffed, equipped unit available at 2 a.m. whether or not anyone calls, a fixed-cost structure that CMS's own analysis for Congress singles out as the industry's defining economics 7. Set against that fixed cost, the public payers underpay: GAO found Medicare reimburses about 6 percent below the average cost per transport 8, Medicaid in roughly half the states pays about half the cost of service, the uninsured account for around 14 percent of transports, and in total EMS agencies collect below-cost payment on roughly 72 percent of everything they do 9. The commercial patient is not paying for their ride. They are paying for the system, one balance bill at a time.
Where consolidated capital found this market, prices confirmed the logic. Among air ambulances, carriers owned by private equity or publicly traded companies averaged allowed amounts of $32,051 per helicopter transport, 5.6 times what Medicare would have paid, roughly 60 percent above every other ownership type 10. Congress looked at that market and acted. It looked at ground ambulances and did something stranger.
The law that stopped at the curb
The No Surprises Act, in force since January 2022, ended balance billing for emergency care, for out-of-network clinicians at in-network facilities, and for air ambulances. Ground ambulances are the one major emergency service it excluded, in part because Congress did not know how to regulate a market made of fire departments, municipal rate ordinances, hospital services, and private carriers all at once. Legal scholars now call ground transport the last gap in the No Surprises Act 11. Instead of closing it, Congress commissioned an answer: the Ground Ambulance and Patient Billing Advisory Committee, which delivered its report to the Secretaries on August 28, 2024 12.
The committee's recommendations are specific and, by surprise-billing standards, elegant. Ban balance billing for ground ambulance services, emergency and interfacility alike. Cap patient cost-sharing at the lesser of $100 or 10 percent of the established rate. Treat ground ambulance as an essential health benefit. Require insurers to pay within 30 days, using a rate hierarchy that respects local control: a state-law rate first, then a locally regulated rate, then a negotiated rate, then a congressionally set percentage of Medicare, with no arbitration process at all, a deliberate break from the No Surprises Act's expensive dispute-resolution machinery 12.
Nearly two years later, Congress has not acted on any of it. The states have moved instead: 22 states now shield patients in state-regulated plans from ground ambulance balance bills, five states acted in 2025 alone, and 13 of the 22 extend protection to nonemergency transport 5,13. The only ambulance bills with real momentum in the 119th Congress, H.R. 2232 and S. 1643, extend rural Medicare add-on payments; they are provider-payment patches, not patient protections 14. And state laws cannot reach self-funded employer plans, which cover roughly 60 percent of insured workers 5. That hole has a single key, and it is federal.
Congress commissioned the answer, received it in August 2024, and has let it sit. The ambulance is now the last major emergency service in America where being insured does not protect you.
Meanwhile, the ambulance is still a black box
Here is the part of the story the billing coverage never reaches. The same underfunded, fragmented structure that produces the surprise bill also produces something quieter: an information blackout between the ambulance and the emergency department. At many hospitals, the sum total of pre-arrival intelligence is still a scratchy radio patch, thirty seconds of one-way summary. There is often no live feed of inbound ambulances, no shared ETA, no transmitted vitals, no image of the ECG. An emergency physician can watch a pizza cross town in real time and cannot see the STEMI eight minutes out.
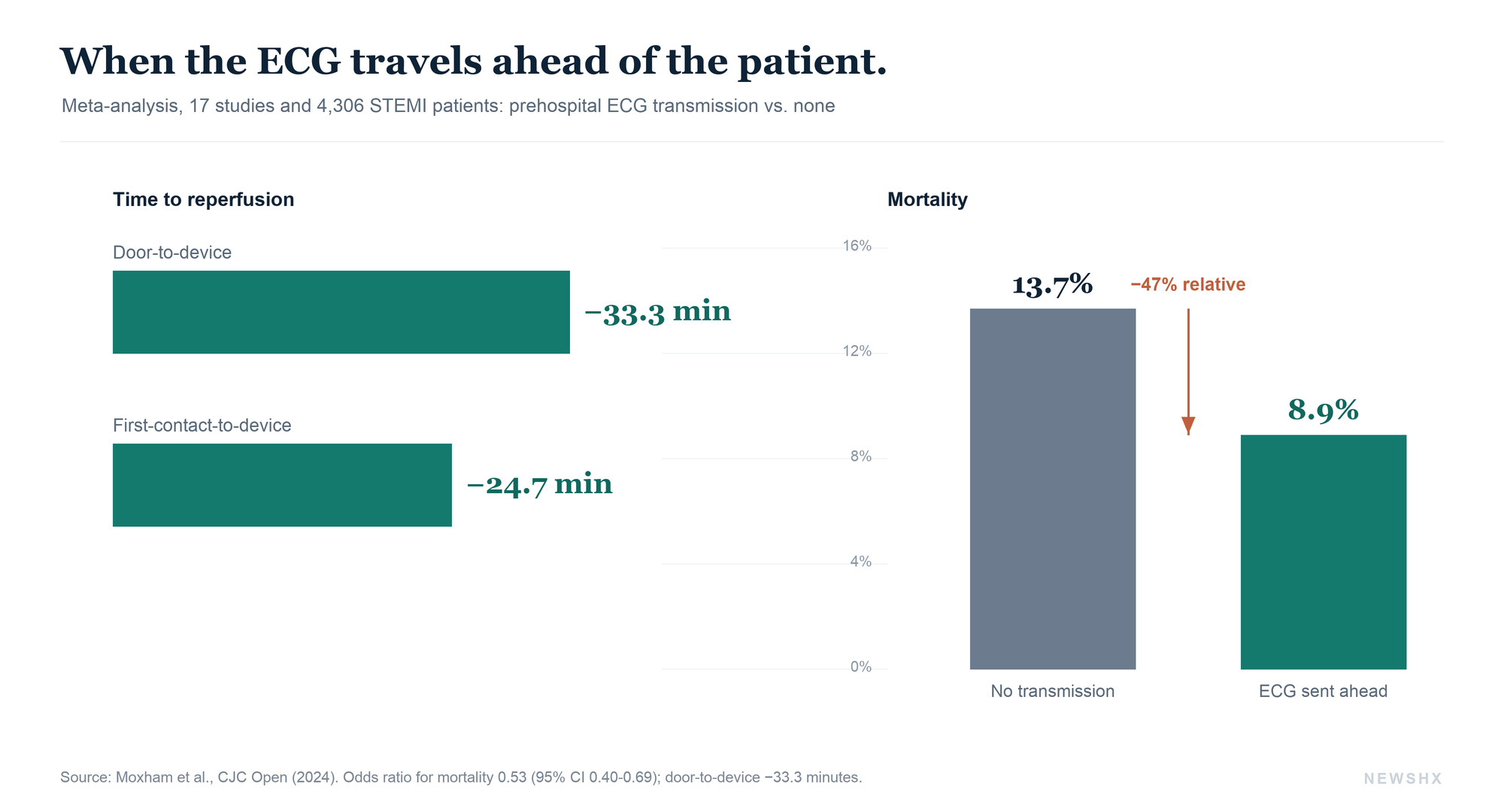
The clinical cost of that blackout has been measured, and it is not small. A 2024 systematic review and meta-analysis, 17 studies and 4,306 STEMI patients, found that transmitting the prehospital ECG to the receiving team cut door-to-device time by 33.3 minutes and first-medical-contact-to-device time by 24.7 minutes, and was associated with a 47 percent relative reduction in mortality, 8.9 versus 13.7 percent 15. An earlier hospital-system study found that simple EMS STEMI notification predicted shorter door-to-balloon times and smaller infarct size 16. Cardiology spent two decades shaving minutes inside the hospital. The largest remaining block of minutes is sitting in the driveway.
None of this requires inventing technology. Pulsara, a shared patient channel that gives EMS and hospital teams live ETA, vitals, and ECG images, has been deployed statewide in Florida by the state health department, at no cost to EMS agencies 17. Twiage, which replaces the radio patch with GPS-tracked arrival feeds and pre-registration data, runs in more than 100 hospitals and health systems including Mayo Clinic and Yale New Haven, and was acquired by TigerConnect in late 2024 18. The obstacle is not the software. It is that nobody pays for the information. There is no reimbursement code for transmitting an ECG ahead of arrival, no payment differential for a documented pre-arrival notification, and 14,000 agencies each deciding alone whether an unfunded data feed is worth it 6.
The blindness runs in both directions, and it continues at the ER wall. The national EMS database now holds more than 378 million records on a modern, standardized format 6, yet hospital outcome data rarely flows back to the crews who delivered the patient. And when the ambulance arrives unannounced at a crowded department, it waits: in California, the mean ambulance patient offload time is 42.8 minutes, and nearly half of local EMS agencies exceed the state's 30-minute standard 19. Every one of those minutes is a paramedic crew standing at a wall instead of covering a district. Which is to say, the readiness everyone is paying so much for, idling in a hallway.
The legislative energy exists. It is just pointed at the pieces separately. State legislatures enacted roughly 370 EMS bills in 2025, with funding sustainability and data modernization among the recurring themes 20, and California now mandates a 30-minute offload standard with required reduction protocols 19. What no bill yet does is connect the two conversations: the payment reform and the data reform are still strangers.
Pay for readiness and information, not mileage
Line the two halves up and the fix stops looking like two fixes. Adopt the GAPB framework federally: take the patient out of the middle, cap cost-sharing, and set a payment floor that reflects readiness, so the below-cost math that drives $1,277 base charges begins to unwind 12. Then attach the data obligation to the new money: a system paid for readiness should be required, and funded, to transmit what it knows before it arrives. A pre-arrival data feed is to the modern emergency department what the prehospital ECG was to the cath lab, and that experiment has already been run. It saved 33 minutes and was associated with nearly half the deaths 15.
Health system leaders do not need to wait for Congress to do the second half. The operational moves are available now: put a shared pre-arrival platform in front of the highest-acuity service lines, wire EMS ETA and telemetry into the ED track board, feed outcome data back to EMS partners, and treat ambulance offload time as a board-level throughput metric, because it is one 19. Every one of those steps makes the most expensive ride in American healthcare worth more than it costs. For the moment, that is more than Congress can say.
For operators: the bill problem needs Washington. The blindness problem does not. Pre-arrival data platforms, offload metrics, and bidirectional EMS data exchange are all buyable today, and the mortality evidence is already in.
A 911 call sets in motion the most capital-intensive house call in medicine: staffed around the clock, dispatched in minutes, priced like a taxi, and communicating like it is 1978. The bill and the blindness grew from the same root. So will the fix.
Disclosure: neither NewsHX nor A3HCS has any commercial relationship with Pulsara, Twiage, TigerConnect, or any other vendor named in this article.
The bill problem needs Washington. The blindness problem needs an operator.
A3HCS works with health systems and EMS partners on the operational half of this story: pre-arrival data platforms and ED track-board integration, ambulance offload throughput, EMS partnership and medical direction strategy, and the payer dynamics behind out-of-network transport. If your emergency department still learns about inbound patients by radio, that is a solvable problem, and it does not require an act of Congress.
Start the conversation at A3HCS.orgReferences
- FAIR Health. Ground Ambulance Services in the United States: A Study of Private Healthcare Claims. FAIR Health White Paper; March 2022. fairhealth.org
- FAIR Health. Nearly 60 Percent of Ground Ambulance Rides Were Out of Network in 2022. FAIR Health study release; 2024. fairhealth.org
- Kaiser Family Foundation. Ground Ambulance Rides and Potential for Surprise Billing. KFF Issue Brief; June 2021. kff.org
- Gong JH, Azad CL, Zhang G, Means KR Jr, Aliu O, Giladi AM. Site of Ambulance Origination and Billing for Out-of-Network Services. JAMA Netw Open. 2024;7(2):e240118. doi:10.1001/jamanetworkopen.2024.0118
- Kelmar P. EMERGENCY: The High Cost of Ambulance Surprise Bills. U.S. PIRG Education Fund; December 2022, state-count updates through February 2026. pirg.org
- NEMSIS Technical Assistance Center. Monthly Activity Report, July 2025. National EMS database: 378.9 million records from 14,157 reporting agencies across 54 states and territories. nemsis.org
- Centers for Medicare & Medicaid Services. Evaluation of Hospitals' Ambulance Data on Medicare Cost Reports and Feasibility of Obtaining Cost Data from All Ambulance Providers and Suppliers: Report to Congress. September 2015. cms.gov
- U.S. Government Accountability Office. Ambulance Providers: Costs and Expected Medicare Margins Vary Greatly. GAO-07-383; May 2007. gao.gov
- National EMS Advisory Council (NEMSAC). Final Advisory: EMS System Funding and Reimbursement. ems.gov
- Adler L, Milhaupt C, Ly B, Trish E. Private Equity-Owned Air Ambulances Receive Higher Payments, Generate Larger and More Frequent Surprise Bills. Brookings Institution; November 16, 2021. brookings.edu
- Petrie-Flom Center, Harvard Law School. Ground Ambulances: The Last Gap in the No Surprises Act. October 16, 2025. petrieflom.law.harvard.edu
- Advisory Committee on Ground Ambulance and Patient Billing (GAPB). Report to the Secretaries of Health and Human Services, Labor, and the Treasury: Recommendations on Preventing Balance Billing for Ground Ambulance Services. Delivered August 28, 2024. cms.gov
- Stovicek N, Hoadley J. Consumers Still Face Surprise Bills for Ground Ambulances; States Are Trying to Protect Them. The Commonwealth Fund, To the Point blog; 2026. commonwealthfund.org
- H.R. 2232 / S. 1643, Protecting Access to Ground Ambulance Medical Services Act of 2025, 119th Congress (2025-2026). congress.gov
- Moxham RN, d'Entremont MA, Mir H, Schwalm JD, Natarajan MK, Jolly SS. Effect of Prehospital Digital Electrocardiogram Transmission on Revascularization Delays and Mortality in ST-Elevation Myocardial Infarction Patients: Systematic Review and Meta-Analysis. CJC Open. 2024;6(10):1199-1206. doi:10.1016/j.cjco.2024.06.012
- Kobayashi A, Misumi N, Aoi S, et al. STEMI Notification by EMS Predicts Shorter Door-to-Balloon Time and Smaller Infarct Size. Am J Emerg Med. 2016;34(8):1610-1613.
- Florida Department of Health. Pulsara Communications Platform: Statewide EMS-ED Communication Program. floridahealth.gov
- TigerConnect. TigerConnect Acquires Twiage, Enhancing Real-Time EMS-to-Hospital Communication for Streamlined Emergency Care. Business Wire; November 20, 2024.
- Feldmeier M, et al. Patterns in California Ambulance Patient Offload Times by Local Emergency Medical Services Agency. JAMA Netw Open. 2024;7(12):e2451022. doi:10.1001/jamanetworkopen.2024.51022
- National Conference of State Legislatures. Funding Stat! States Secure Timely Support for EMS Systems. NCSL; 2026. ncsl.org