
Most people in healthcare think a career is about building a ceiling. How high can I climb? What is the most impressive version of this work I can build from the credentials and the hours I put in?
When you build a ceiling, people can see it. The title on the badge. Chief of something. The corner office on the administrative floor, away from the units. The keynote invitations, the board seat, the parking spot with your name on it. From the outside, a career like that looks like you have arrived.
But I have come to learn, slowly and usually the hard way, that the people who last in this field, the ones who still have something left for their patients and their families at sixty, are rarely the ones who chased the ceiling. They built a floor instead. A floor is what holds you up when something goes wrong. And in medicine, something always goes wrong eventually. A bad outcome. A lawsuit. A restructure that erases your department on a Tuesday. A termination that always lands on a Friday. A body that finally sends the bill for fifteen years of nights and skipped meals.
A ceiling is what you show people. A floor is what catches you. We have built an entire system that rewards the first and refuses to pay for the second.
The climb feels like safety. It is not the same thing.
I spent the early part of my career certain the ceiling was the point. You watch the attendings with the titles, the administrators with the influence, and you tell yourself that is what winning looks like. So you take the extra service line. You say yes to the committee. You let the work expand until it fills every hour you have, because climbing feels like progress, and progress feels like safety.
Here is what raising the ceiling actually looks like from the inside. You optimize yourself the way a hospital optimizes a balance sheet. More volume. More throughput. More RVUs. You become very good at producing the metrics that get you promoted, and you tell yourself the cost is temporary. The marriage will keep. The sleep will come back. The version of you that had friendships outside the hospital is just on pause until you reach the next rung.
And then one day the bill arrives, and it is not sitting in your driveway on four wheels. It is sitting in your chest at three in the morning. It is the colleague who was the most impressive clinician any of us knew, who walked out mid-shift one morning and never came back, because the floor underneath all that achievement had quietly rotted through. Nobody saw it, because nobody can see a floor. You can only see the ceiling.
The workforce crisis is a floor that was never poured
This is the part of the workforce crisis we keep getting wrong. We talk about it as a staffing number, a vacancy rate, a recruitment problem. It is not. It is thousands of people who were handed a ladder and never a floor. We told an entire generation of clinicians to climb, and we built systems that reward the climb, and we are genuinely surprised when they fall and there is nothing underneath to catch them. The U.S. Surgeon General named health-worker burnout a national crisis, and the National Academy of Medicine put a system, not a personality, at its root. 1,2
A floor for a healthcare worker is not glamorous, which is exactly why almost nobody builds one on purpose. It is boundaries you actually hold. It is enough financial margin that you are not trapped in a toxic job, so you can say no to the wrong system the way you would say no to the wrong client. It is a second skill that does not depend on one employer's mood. It is protecting your license and your name before you protect your image. It is the relationships and the sleep that no org chart can take from you in a reorganization. None of it gets announced at the leadership retreat. You feel it only when something breaks, and then you feel it every single day.
I have watched two kinds of people go through the same career shock, the same lawsuit, the same merger that eliminated their role. The ceiling builders panic, because the title was the whole structure, and when it goes the structure goes with it. The floor builders absorb it. Some of them even see the opening, the way a careful investor sees a market crash as a buying opportunity instead of a catastrophe. The difference was never talent or income. It was what they had positioned underneath themselves while everyone else was busy reaching up.
The same blindness runs all the way to the patient
The same logic runs straight through to the patient, which is the part I cannot let go of, because my work is in brain injury and recovery, where the floor is the entire game.
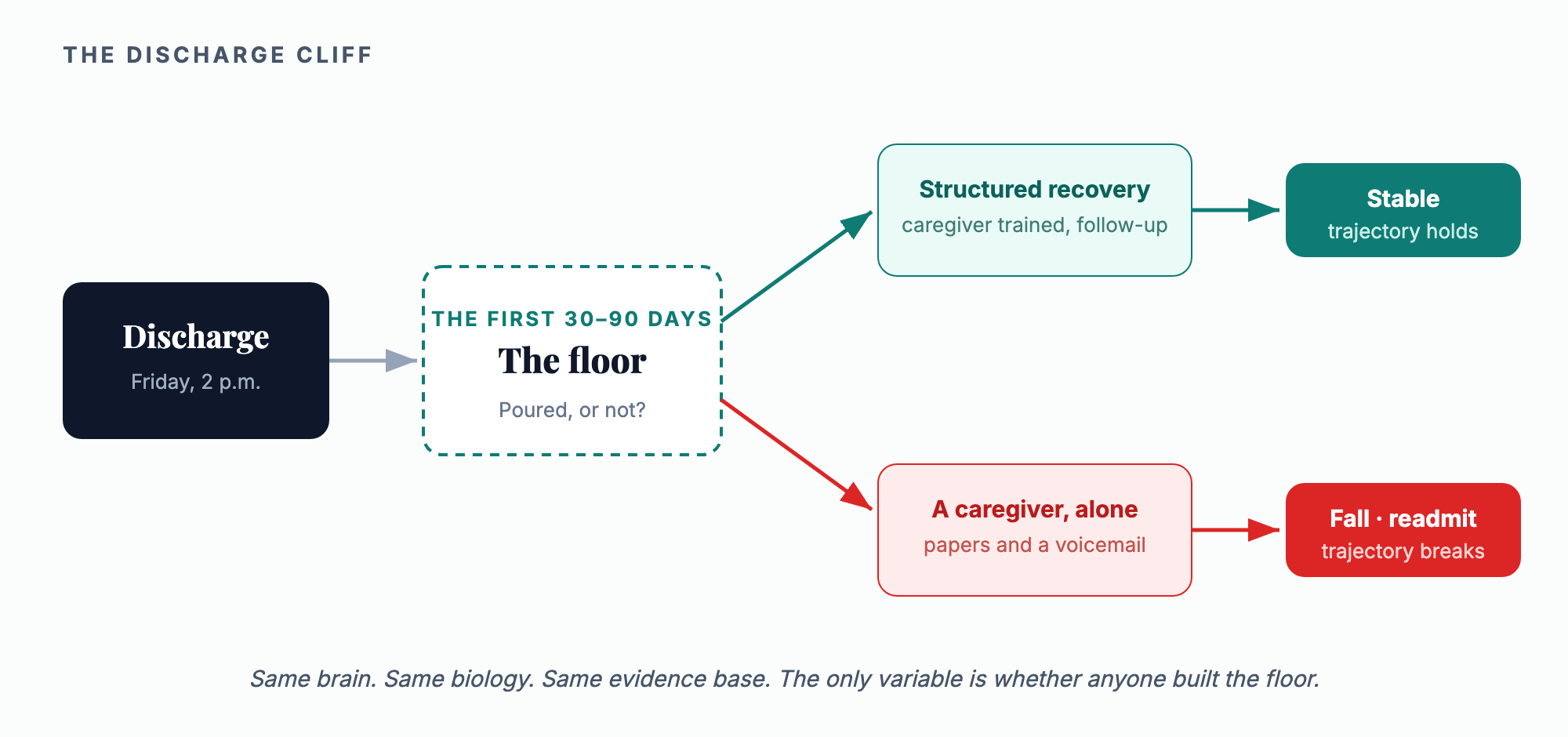
A hospital builds its ceiling in public. The new tower with the donor's name on it. The robotic surgery suite. The advertised volumes, the rankings, the ribbon cuttings. That is the visible, fundable, impressive part. And then the patient with a traumatic brain injury gets discharged on a Friday afternoon into a floor that was never built. There were 214,110 TBI-related hospitalizations in the United States in a single recent year, and the survivors go home up to four times more likely to fall than their peers, into the exact window where the system goes quiet. 3,4 A caregiver is handed a stack of papers and a phone number that goes to voicemail. The gap between the ceiling we celebrate and the floor we never funded is precisely where people fall.
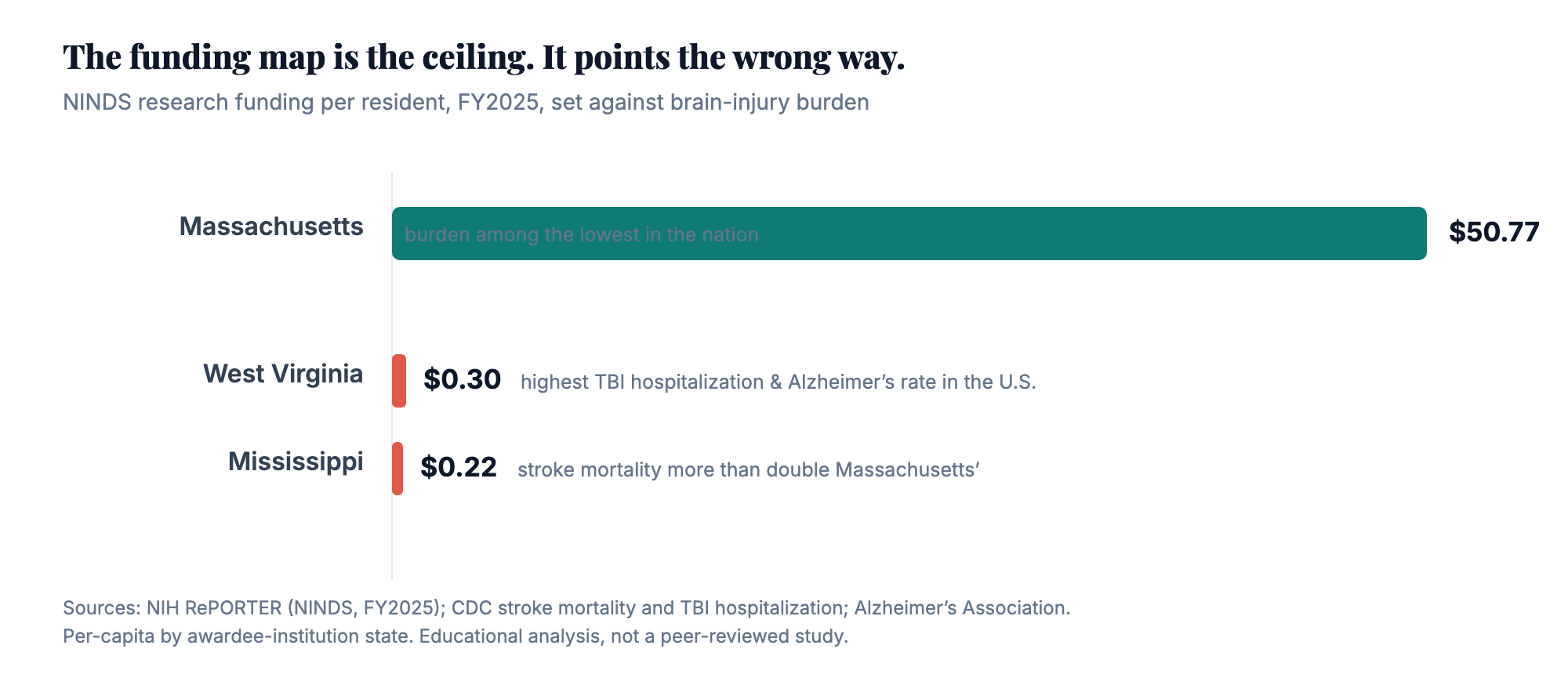
And the system is built upside down at the largest scale, too. Federal neuroscience research, the ultimate ceiling, concentrates where the research towers already stand. In FY2025 the nation's neurological institute awarded roughly $2.55 billion, and per resident it lands like this: Massachusetts receives about $50.77 a person; Mississippi, with more than twice the stroke mortality, receives 22 cents; West Virginia, which carries the highest TBI hospitalization rate and the highest Alzheimer's prevalence in the country, receives 30 cents. 5,6,7,8 The places where brains are most at risk are the places the research engine touches least.
The reframe leaders can act on this quarter
Let me be precise, because the lazy version of this argument deserves to lose. Research concentrates where infrastructure exists, and peer review rewards capability, as it should. Nobody serious is proposing we apportion grants by ZIP code. The research engine is working as designed. That is exactly the problem: the system has no second engine. We built a world-class machine for discovering how the brain heals and almost no machine for delivering what we discover to the people doing the healing.
Your state's position on the funding map is not your constraint. Your discharge process is. A hospital cannot become a top-ten NIH recipient this year. It can make sure every stroke and TBI patient leaves with a structured 90-day recovery plan, a trained caregiver, and scheduled follow-up through the window where falls and readmissions actually happen, and it can pour a workforce floor on the staff side: a budgeted behavioral-health and recovery program, not a wellness email.
That is not research. It is translation, and it is the cheapest high-yield intervention in neurology. It works anywhere there is an internet connection, which is rather the point. Consider the scale of the floor we are not pouring: 214,110 TBI hospitalizations a year, survivors going home up to four times more likely to fall, and a 30-to-90-day window where the support that changes trajectories is most needed and most often missing.
The bottom line
Neither instinct is wrong on its own. Ambition is not a sin, and building a ceiling feels like the whole point when you are working hard and you are good at it. I reached. I reach now. But I feel fortunate that I learned the difference earlier rather than later, before the bill came due, because the people who learn it too late tend to learn it the hard way, in a hallway, in a divorce, in a body that quit on them, or in a patient who fell through a gap we could have closed.
So this week I am asking you to look down. Not at the title, not at the version of your career or your hospital that looks good on a conference badge, but at the floor underneath all of it. If the job disappeared tomorrow, if the body or the name took a hit, if the patient went home on a Friday, would it hold? Nobody is ever going to compliment you on your floor. There is no award for it and no ribbon cutting. But you will feel it, in your sleep and in your nerve and in your patients' outcomes, every single day.
Is your system building a ceiling, or pouring a floor?
A3HCS helps health systems and post-acute operators build the floor that holds: care-transition and discharge processes that protect patients through the dangerous first 90 days, and a workforce strategy that treats clinician health as infrastructure, not a perk. For the patient side, Brain Revives (brainrevives.com) delivers physician-led recovery education for the post-discharge window the system abandons.
Build the floor with A3HCS.orgReferences
- Office of the U.S. Surgeon General. Addressing Health Worker Burnout: The U.S. Surgeon General's Advisory on Building a Thriving Health Workforce. U.S. Department of Health and Human Services; 2022.
- National Academies of Sciences, Engineering, and Medicine. Taking Action Against Clinician Burnout: A Systems Approach to Professional Well-Being. Washington, DC: The National Academies Press; 2019. doi:10.17226/25521.
- Centers for Disease Control and Prevention. Traumatic Brain Injury & Concussion: surveillance data (214,110 TBI-related hospitalizations, United States, 2020). Accessed June 21, 2026.
- Brain Revives. Conditions: brain-health burden, elevated fall risk after brain injury (up to 4x), and the 30-to-90-day post-discharge recovery window (underlying fall data: CDC STEADI). brainrevives.com/conditions. Accessed June 21, 2026.
- National Institutes of Health. NIH RePORTER: National Institute of Neurological Disorders and Stroke (NINDS) awards, FY2025 (~$2.55 billion). reporter.nih.gov. Accessed June 21, 2026.
- Brain Revives Brain Health Map. NINDS FY2025 awards aggregated by awardee-institution state, per capita (U.S. Census 2024 population estimates). brainrevives.com/brain-map. Accessed June 21, 2026.
- Centers for Disease Control and Prevention. Stroke mortality, age-adjusted death rates by state (adults 35+); Interactive Atlas of Heart Disease and Stroke. Accessed June 21, 2026.
- Alzheimer's Association. 2024 Alzheimer's Disease Facts and Figures (state prevalence among adults 65+; West Virginia highest). Alzheimers Dement. 2024;20(5). Accessed June 21, 2026.